In the last “Tricks of the Trade” column (November 2016), we reviewed how to use end-tidal capnography to detect diabetic ketoacidosis and monitor chronic obstructive pulmonary disease exacerbations. Now we’ll explore using end-tidal capnography to check orogastric/nasogastric tube placement and guide cardiopulmonary resuscitation.
Explore This Issue
ACEP Now: Vol 35 – No 12 – December 2016Using End-Tidal to Check Orogastric/Nasogastric Tube Placement
Press Ganey scores likely skyrocketed once we stopped shoving nasogastric tubes (NGT) into every patient with the slightest evidence of an upper gastrointestinal bleed, but we are still placing orogastric (OGT) or NGT in our intubated patients in the emergency department. While insertion of these tubes is a relatively straightforward procedure, it can result in fatal consequences if there is inadvertent airway placement of the tube. This dire misplacement is even possible in intubated patients with an inflated endotracheal cuff.1,2 Typically, we check for aspiration of stomach contents and auscultate to confirm placement, but these can be unreliable indicators, especially in a busy emergency department.3 The gold standard for tube placement is visualization of the tube passing below the diaphragm on chest X-ray, which you could be waiting up to 87 minutes to receive.4,5
In theory, end-tidal capnograms are used to determine whether patients are hypoventilating, leading us to believe that using end-tidal to check for unintentional pulmonary placement of NGT/OGT should be effective. With the increasing availability of end-tidal capnometry in the emergency department, it is convenient enough to temporarily attach one to the NGT/OGT (see Figure 1).
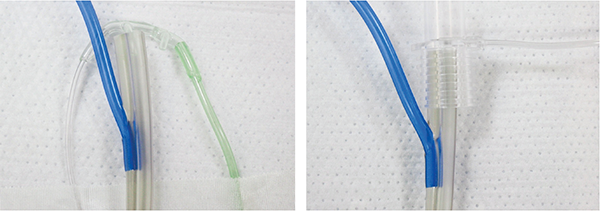
Figure 1. Placement of a Side-Stream Capnometer (left) and Mainstream Capnometer (right)
Meyer et al demonstrated that in 100 mechanically ventilated patients, a colorimetric capnometer was able to exclude tracheal placement 100 percent of the time.4 In this study, an NGT was initially inserted to a depth of 30 cm and insufflated and exsufflated with 50 cc of air, then the end of the tube was capped with the colorimetric capnometer. If the color remained purple, indicating an end-tidal CO2 (EtCO2) 15 mmHg, the tube was removed. In a meta-analysis of nine clinical trials of mechanically ventilated patients, the use of either qualitative or quantitative capnometry for tracheal placement of the NGT had sensitivities ranging from 88 to 100 percent and positive likelihood ratios of 15.2–283.5.6 Before your patient leaves the emergency department, a chest X-ray is needed to confirm placement of your NGT/OGT, but end-tidal capnography can help to avoid accidental airway insertion, multiple attempts at placement, and multiple chest X-rays. (See Figure 2 for an algorithm for placing NGT/OGT.)
Pages: 1 2 3 4 | Single Page




No Responses to “Use End-Tidal Capnography for Placing Orogastric, Nasogastric Tubes, and CPR”