Explore This Issue
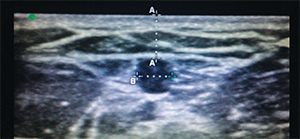
ACEP Now: Vol 33 – No 12 – December 2014Figure 5. A vessel within the parameters for optimal depth and width for catheter placement.
5 Place the Ultrasound on Shallowest Depth for the Vascular Probe
The peripheral veins regularly targeted for ED catheter placement are often superficial. There will be times when the only available vein runs deeper. It is important to remember that the deeper the targeted vein, the lower your success rate for placing an intravenous catheter. A 2010 observational study in The Journal of Emergency Medicine found that success rates were significantly higher for veins of moderate depth between 0.3 cm and 1.5 cm.7 In the same study, the authors found that depth was not the only measurement that predicted success rates of intravenous catheter insertion. Successful cannulation also vastly improved when the targeted vein diameter was greater than or equal to 0.4 cm2. Figure 5 shows a vessel within the parameters for optimal depth and width based on this study. Placing the ultrasound on the shallowest depth not only encompasses this range, it also narrows the field to those veins with higher success rates. The shallow depth with the vascular probe also allows for an expanded view of the targeted area, allowing for better visualization of the beveled edge of the catheter. When inserting the catheter through the patient’s skin, be sure to keep the bevel tip facing up to allow the ultrasound beam to strike the beveled edge. When the ultrasound beam strikes the beveled edge, it creates artifact that allows for easier visualization of the tip as you cannulate the vein.

Figure 6. Short-axis positioning.
6 Short Axis Versus Long Axis Approach
The ultrasound probe for intravenous catheter placement can be positioned on two axes, short or long. There are no studies to support greater success with one axis over another, but familiarity with both approaches may help to improve your visualization in real time. In short axis (see Figure 6), a trick to improve visualization of the catheter as you advance through the soft tissue toward the targeted vein is the “tilt to follow” method. Once the target vein is located, tilt the probe so the sonographic beams are angled toward the catheter at initial insertion. Then follow the catheter toward the vein, tilting the probe away from you toward the direction of the catheter as it passes beneath your initial position to a position distal to where the catheter will penetrate the venous wall. Using the “tilt to follow” method will limit the likelihood of advancing the catheter through the posterior venous wall, causing extravasation (see Figure 7). Another approach using the long axis gives you a longitudinal view of the entire length of the targeted vessel (see Figure 8). The sonographic beam is narrow, so you will need to place the catheter tip adjacent to the probe and advance the catheter in the same direction as the probe to be able to follow the beveled tip into the targeted vein.



5 Responses to “10 Tips for Ultrasound-Guided Peripheral Venous Access”
December 13, 2016
Cindy TeslerI agree that intravenous access is a simple procedure that is very important for emergencies. You also said that sometimes, getting access to veins can sometimes be difficult and you need the help of an ultrasound machine. I think it’s a good idea to make sure that the patient is calm and understands what to expect so that you have the best chance of successfully accessing the vein.
December 21, 2016
JordanAgreed. Often times these patient have had several IVs attempted on them already so even acknowledging that and then reassuring them that you will look to find the best possible access point before even attempting to stick them makes a huge difference. Realistic expectations are also important as well as knowing your limits and utilizing a more experienced provider or a PICC team for a midline if available.
June 7, 2017
Ahmed AbdelgawadI think the differences in study results are due to the differences in the experience of the ultrasound procedure operator. In our hospital we can see this clearly. we have a range of 50% up to 99% success rate in the first attempt according to the operator.
July 10, 2017
Dr Aung Htet, MyanmarScanning and locating the vein at the center of probe in short axis view
and inserting needle at the center is a useful method. But there will be some difficulty if there is no center marking on the probe.
Another useful trick is place the vein at the corner of the probe in shortaxis and enter the needle over that corner. Moving the needle in the soft tissue towards the vein will be oriented by correct screen-to-patient orientation of probe.
March 12, 2019
james maxwellI’ve been using US for iv placement for about 8 yrs now. Been an RN for 15 years, am currently a flight RN, have 3yrs ICU experience, 13yrs ER experience, and 1.5yrs of PICC team experience. US for iv placement is an invaluable skill in the critical care setting and as you become proficient you will realize that you can use this skill very effectively in nearly all areas of the ER (including very critical situations)
—here are my tips for someone interested in becoming proficient in using US for iv placement
a) start by going to youtube and watching the video: Ultrasound guided peripheral iv course by siegfried meme.
b) if you don’t have someone on your unit to teach you, shadow your picc team and watch them and pick their brains.
c) familiarize yourself with your units ultrasound machine. focus on the probe(which one to use and how to select it), depth adjusters, and gain.
d) practice! don’t expect to get good if you don’t practice. there are arm models out there. your unit may have one-the picc team may have one. maybe you can get your unit supervisor to order on out of your budget. practice on it. learn to trust that what you are seeing on the screen is what is happening at your fingertips.
e) when you start using US on actual pts, don’t start on legitimately HARD pts; your chance of success will be low and your rate of frustration will be high. start on people you would normally have no problem with getting a traditional iv on. explain to them why you are using US and if they are ok with that. if you have someone there already trained, has them shadow you and ready to step in and take over if you have problems.
f) develop a routine and do it the same every time. you will find that this will save you tons of time in the long run and it will even increase your success rate.
g) selecting the appropriate catheter-VERY IMPORTANT!!! the more catheter in the vessel = less chance of infiltration. unless it is a very superficial vein ( 0.5cm in depth. Kiddos have very elastic vessels which can actually be hard to penetrate. if the depth is good and the vessel is good and straight, don’t be afraid to use a 1.75″ catheter. for infants, i usually use a standard 1″ 22ga catheter. i very rarely use a 24ga b/c they are simply too short (unless its a primi)
h) thoroughly assess the vessel you are going to access. track it up at least the length of the catheter you are going to use. look for any bifurcations or sudden changes of direction which may prevent successful cannulation of that vessel. this includes assessing both arms if you are not completely confident in what you see the first time. take your time!
i) MARK YOUR SPOT! i can’t emphasize this enough! i use the tip of the catheter cover. after orienting your probe and locating your vessel, compress w/the catheter cover on both sides of the vessel until you are certain you are over the vessel. when you are, push down w/enough pressure to leave an indentation. this is your point of entry. if you get in the habit of doing this you’ll find that 9x out of 10 you are right over the vessel (this helps in locating the tip on US before you access the vessel).
j) USE LIDOCAINE! 1%-2% buffered if available but otherwise as is. this procedure relies on being slow and steady. movement of any kind is your enemy and you are doing this w/a sharp object going thru someones tissues. be humane and use lidocaine every time (unless the pt specifically refuses). inject at the middle of the indentation to produce a SQ bleb.
k) locate the tip of needle on US. to become good at this takes practice (see d above). this involves moving the probe and knowing the limitations of the probes field of view (i.e. if you just keep advancing the catheter and don’t move the probe accordingly, you’ll pass beyond the what the probe can “see” and will be advancing the catheter blindly). if you are having a hard time initially seeing the catheter, stop, withdraw the needle just a little bit, wiggle it, and start to advance again and try to see it with the probe.
l) flash does not mean advance the catheter off the needle (a common mistake i see w/many people)! flash means you punctured the vessel wall and nothing more. now you need to locate the tip and orient it to the center of the vessel. once you do that you need to advance the tip while keeping track all the time with the probe. this is where trusting what your seeing on the screen is what is happening at your fingertips. there is absolutely no reason to take your eyes off the screen and look down. after you have located the tip and it’s oriented in the middle of the vessel, advance it until you don’t see it on the screen. NOW STOP advancing the catheter! now move the probe up until you see it again and hold the probe there. repeat this “leapfrog” method 2-3 times before you put the probe down and finish with your cannulation. for really hard pts, sometimes i will use this leapfrog method until the entire catheter is hubbed (that way there is no doubt you have access).
m) short axis (cross cut) view vs long axis view and the “wiggle” test. i use the short axis exclusively. using the long axis is useful i suppose if you want to see how much of the catheter is in the vessel but if you’re really that concerned then you probably didn’t use a long enough catheter or you tried to access too deep of a vessel to begin with. use the short axis view and get good at finding the tip and that is all you will need to ensure successful cannulation. the “wiggle” test is mentioned by some as a way to see if you are in the vessel-find the tip and you’ll know exactly where you are.
n) BE CLEAN!!! too many times i see people using non sterile gel or being careless with the probe. use sterile lube only! when handling the probe, do not allow the sterile tegaderm covered probe to touch anything!
o) stay away from brachial veins and upper vessels w/the exception of upper cephalic veins. learn your anatomy. ONLY use brachial veins (in forearm and above the elbow) when you are 100% confident in your skills!!! as far as the upper vessels go, if you must, ONLY use 6.4cm long catheters and be very cautious of accessing vessels >2cm in depth. remember that when using these vessels you need to account for actual distance to the vessel as well as compression of the tissue when locating the vessel. remember that if you cause an extravasation in an upper vessel, you have put that limb out of commission until the infiltration has resolved (this includes using that extremity for PICC placement). i find these situations mostly arrive at night when resources are more limited. If you find yourself in this position and the pt is truly critical, it is best to get your MD to place a central line.
p) KIDDOS-once you get good you’ll find yourself looking forward to those crazy tense moments of starting pedi ivs b/c you know you’ll most likely get it the first time and you’ll be able to choose where to put it. for kiddos, find your spot and if time permits, use LMX if available and then inject lido to “double numb” the area. the most important part of starting pedi iv’s is the holder(s). i won’t go into all that but just remember that and when the time comes you’ll know how to describe how you want them to hold them.
q) hav fun and keep track of your starts. starting us iv’s is one of my favorite things to do. you’re providing a service that truly reduces pt anxiety and helps them. your co-workers will absolutely appreciate you and look to you first to help get that hard stick. keep track of those stats and you’ll be amazed how good your success rate can become. you’ll find that 9x+/10x success rates the “first time” are realistic and that you’ll very rarely be unable to gain access. GOOD LUCK!!!