
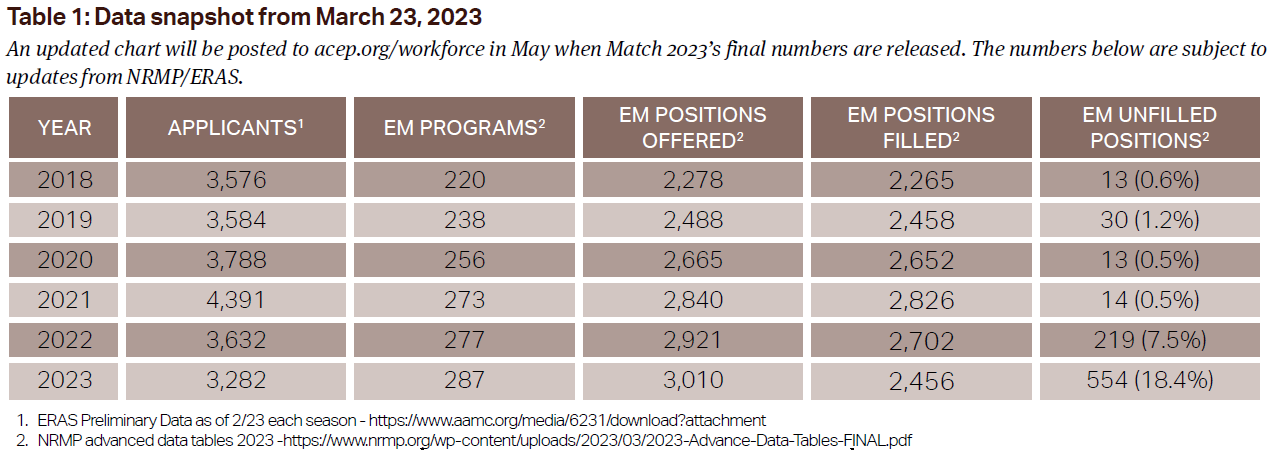
For decades, emergency physicians took pride in being a much-desired specialty for graduating medical students. Emergency medicine residencies routinely filled 99 percent of their available positions in the Match. On Monday, March 13, 2023, 554 emergency medicine spots went unfilled, a dramatic and abrupt increase in just a couple of years. The majority of those spots were filled by March 17 during the National Resident Matching Program’s Supplemental Offer and Acceptance Program (SOAP), but the final data won’t be released until May.1,2
Explore This Issue
ACEP Now: Vol 42 – No 03 – March 2023, ACEP Now: Vol 42 – No 04 – April 2023Emergency medicine’s desirability among medical students has dramatically decreased over the past two residency application cycles, falling below the number of applicants who applied to emergency medicine before the onset of the COVID-19 pandemic. U.S. student applicants to emergency medicine residencies accredited by the Accreditation Council for Graduate Medical Education (ACGME) and the American Osteopathic Association (AOA) dropped by 16.8 percent from 2021 to 2022.1 In the 2023 residency Match year, emergency medicine applicants dropped by an additional 18.1 percent. In this article, we explore key reasons for the abrupt decrease in the competitiveness of the emergency medicine Match and recommend changes the specialty can undertake to reverse this trend.
The 2021 Match results marked a change for the specialty. However, long-term challenges such as night shifts, intoxicated patients, and the administrative burden of emergency medicine residents cannot explain the recent change in medical student preferences. The decrease in applications for emergency medicine residencies is specialty-specific. While total residency applications grew at a steady rate and other specialties have faced the same COVID-19 pandemic and similar nursing workforce shortages, they did not see the same declines in applications that emergency medicine has witnessed.
Click to enlarge.
There are many speculations about what caused this shift. Like most things, the origins are likely multifactorial and still evolving. There are certainly many challenges facing the emergency physician today including workforce concerns, emergency department (ED) boarding, the impact of the COVID-19 pandemic, the corporatization of medicine, and violence directed toward health care workers, among many others.
The Shifting Emergency Medicine Workforce
In March 2021, eight emergency medicine organizations released the “Emergency Medicine Physician Workforce: Projections for 2030” report with its data published in the December 2021 issue of Annals of Emergency Medicine.3,4 The report painted a startling picture for the future jobs of emergency physicians. The analysis’s base “scenario would result in a surplus of 7,845 emergency physicians in 2030.” After seeing residents face unprecedented challenges finding attending jobs in 2020 and 2021, medical students were faced with the prospect that job shortages were not just a one-time, pandemic-related problem, but a systemic problem in emergency medicine.5
Details within the workforce projections were especially concerning for future emergency physician prospects. While emergency medicine residency graduates had been increasing by 3.5 percent per year over the past decade, the number of physician assistants (PAs) and nurse practitioners (NPs) working in emergency medicine had been increasing by six percent per year.5 Between 2013 and 2019, the number of PAs and NPs working in emergency medicine practices increased by 48.4 percent, compared with an increase of 11.1 percent for physicians.6 Since PAs and NPs earn significantly less than residency-trained physicians, the prospect of being pushed aside by lower-skilled, lower-cost professions may have driven some medical students to choose other specialties.
Back-to-Back Burnout Champions
Concurrent with predictions of career insecurity for emergency physicians, the job became more difficult and less fulfilling. In the 2018 Medscape Physician Burnout Report, 45 percent of emergency physicians reported being burned out.7 By 2023, the percentage who reported burnout increased to 65 percent, five percent higher than any other specialty. As emergency physician burnout rises, there has been a corresponding increase in emergency physician attrition.8 A recent survey of all physicians (not just emergency medicine) by the Massachusetts Medical Society showed that 50 percent of physicians plan to reduce their clinical workload by June of 2023, and about 25 percent plan on leaving medicine in the next two years.8
The underlying cause of EM’s burnout crisis stems largely from moral injury, the “social, psychological, and spiritual harm that arises from a betrayal of one’s core values, such as justice, fairness, and loyalty.”9 Delivering high-quality patient care in the ED has always been challenging. But in America’s post-pandemic health care system, it has been nearly impossible.
Over the last two years, decreased hospital staffing has caused increased ED boarding nationwide.10 Already under-resourced EDs were tasked with caring for admitted patients in addition to incoming ED patients. That led to ED patients waiting for prolonged periods, becoming frustrated, and suffering adverse outcomes. Dr. Laura Haselden, MD, MPM, an emergency physician in Virginia, opined on Twitter, “The number of times I’ve said, ‘I don’t want to teach you to practice waiting room medicine but it’s what we’ve got,’ probably didn’t help sell anybody.” The sickest patients, often needing transfer to higher levels to care, were stuck in community EDs where emergency physicians did their best, knowing the care being delivered was substandard. Meanwhile, hospital administrators have been depositing ever-increasing paychecks.11
Prior to the pandemic, many emergency physicians could turn to a closely knit group of nurse and clinician colleagues for support. However, 2021 and 2022 saw an unprecedented level of nursing turnover.12 At the same time, emergency medicine groups were rapidly consolidating, fraying bonds previously formed within smaller partnerships.13
Low Money, More Problems
While emergency physician job security and career satisfaction were being eroded, so were our financial prospects. In the 2017 Medscape Physician Compensation Report, 68 percent of emergency physicians reported feeling fairly compensated, the highest among the specialties surveyed.14 By the 2022 survey, only 53 percent of emergency physicians reported feeling fairly compensated, a decrease of 15 percentage points.15 Compensation no longer matches the rigors of the profession.
These compensation headwinds have come from several sources. Because of sales of emergency medicine practices to consolidators, such as private equity firms, emergency physicians now have the lowest rate of practice ownership among the specialties surveyed by the American Medicine Association (AMA).16 The No Surprises Act, passed in 2021, has limited emergency medicine groups’ bargaining power with private insurers.17,18 Simultaneously, government payers have been chipping away at physician reimbursement.
Correcting Course
Emergency physicians, who are trained to improvise and make the most of difficult situations, will need to rely on that ingenuity to reverse these workforce challenges. Many of the factors impairing emergency medicine’s desirability to medical students—such as boarding—are out of an emergency physician’s control. However, much can be done by emergency physicians to improve the specialty’s popularity.
The most important step is to balance the supply and demand for emergency physician labor. Counterintuitively, decreased interest by medical students is actually beneficial in this process. In the 1990s, when anesthesiology experienced a significant drop-off in medical student interest because of the increased use of certified registered nurse anesthetist (CRNAs), the number of available U.S. anesthesia residency positions decreased by almost a third.19 As emergency medicine organizations lack the power to shut down residency programs, decreases in applicants are likely the most effective mechanism for right-sizing the number of emergency medicine residents.
The rapid increase in PAs and NPs working in EDs can also be tempered by emergency medicine’s physician leaders. While individual employer groups are incentivized to hire low-cost, less trained clinicians, the specialty’s national organizations can push back on hiring practices that harm ED patients and physicians. For example, ACEP is planning to expand its ED accreditation programs.20 Just as the American College of Surgeons would not accredit a Level I trauma center that did not staff the correct set of board-certified physician specialists, ACEP’s accreditation can ensure that PAs and NPs are not managing higher acuity patients without proper post-graduate training and active real-time supervision.
The supply side, of physicians, can also be addressed. Traditionally, most emergency physicians have practiced general emergency medicine rather than a subspecialty. However, academic emergency-medicine programs should increase emergency physicians’ access to fellowship training in pain, geriatrics, psychiatry, critical care, and other subspecialties. Emergency medicine leaders must create workplaces more conducive to emergency physician career fulfillment. Moral injury can be addressed by advocating for policies that promote high-quality emergency care. For example, psychiatric boarding is a scourge that can be addressed through increasing state-level behavioral health funding.
Establishing financial incentives for hospitals to improve flow can lead to significant downstream improvements.21 EDs will likely continue being hospital dumping grounds until hospital administrators have financial incentives to move patients out of the ED.22
Clinical autonomy can be encouraged by granting ownership to emergency physicians. Ownership matters; no one washes a rented car. Even private equity firms have the ability to grant ownership stakes to their physician employees.23
Promoting employer competition for emergency-physician labor would incentivize improved working conditions. Currently, crucial information regarding potential alternative workplaces, such as staffing ratios and compensation, is difficult for physicians to find. The information asymmetry decreases physicians’ negotiating leverage and lowers the likelihood that physicians will change jobs. This stagnant marketplace suppresses employers’ incentive to improve and offer competitive compensation. Noncompete clauses similarly hamper flexibility for the physician workforce.
Every system is perfectly designed to get the results it gets.24 We strongly believe that emergency medicine is a great specialty with a powerful mission, and many medical students agree. There were numerous posts on social media by medical students who received notification they had indeed matched in emergency medicine and were excited for their future.
While many were excited to join the specialty, its workforce structure and clinical climate no longer appeals to many graduating medical students, which has resulted in decreased applications for emergency medicine residencies.
 Dr. Adelman is cofounder and chief executive officer of Ivy Clinicians. Dr. Fisher is ACEP’s Senior Director for Workforce and EM Practice. Dr. Dark is the medical editor-in-chief of ACEP Now.
Dr. Adelman is cofounder and chief executive officer of Ivy Clinicians. Dr. Fisher is ACEP’s Senior Director for Workforce and EM Practice. Dr. Dark is the medical editor-in-chief of ACEP Now.
Pages: 1 2 3 | Single Page



One Response to “Unpacking the 2023 Match Week”
March 19, 2023
dr. suziextremely well written- accurate, upsetting and right on point