Physicians, nurses, and staff in emergency departments (EDs) across the country have encountered workplace violence for years. According to federal labor statistics, the prevalence of workplace violence in health care is increasing (see Figure 1). While staff exposure to this violence varies, literature shows nurses are most frequently exposed, with up to 90 percent having experienced workplace violence in their ED careers.1,2 In a 2018 study by ACEP, nearly half of emergency physicians polled reported a physical assault while at work.3 Solutions focused on security or law enforcement responses have not improved these statistics because they fail to address the root causes of workplace violence. For the safety of staff as well as patients, interventions that interrupt escalations before they blossom into violence deserve further study.
Explore This Issue
ACEP Now: Vol 42 – No 11 – November 2023
FIGURE 1: Number of nonfatal workplace violence injuries and illnesses with days away from work, 2011-18. (Click to enlarge.)
The Story in Data
Violence experienced in the ED is often due to agitated, confused, or delirious patients. A study done at the University of Kansas found that approximately 10 percent of the ED volume at a local county hospital was attributed to some type of behavioral emergency and that approximately one in eight ED visits in the U.S are caused by a behavioral crisis.4 As with other daily challenges in the practice of emergency medicine, EDs deserve a range of nuanced, effective tools that can be tailored to particular patients and scenarios. Unfortunately, the science has thus far lagged behind the ballooning behavioral need.
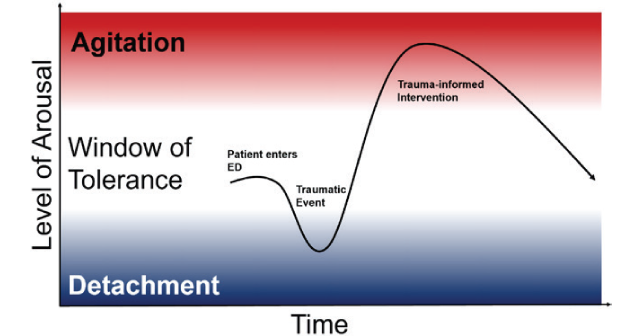
Managing and caring for aggressive patients may involve calling for security or physical and chemical restraints, but these interventions are temporary and have potential to further harm patients physically and mentally.5 Hospitals commonly activate a “code” in response to agitated patients, alerting security personnel to the location of that patient. The difficulty with this approach is that these officers often lack the skills and context needed to de-escalate complex behavioral crises. A study from Australia sought to understand security personnel’s experiences responding to agitated patients in the ED: they frequently felt that they lacked information, coordination, and communication when responding with urgent assistance.6 While the presence of officers can be comforting to staff, it can also be triggering to patients. Security and law enforcement officers can further amplify a patient’s stress response. As additional stress reactions are activated, the window of tolerance for a patient experiencing a traumatic response narrows, increasing the likelihood of escalation.7
Pages: 1 2 3 | Single Page




No Responses to “A Safety Solution for Emergency Department Staff and Patients”