In emergency medicine, the quality of pain management of the acutely injured patient has steadily matured over the past two decades. Instead of a strategy that leaned heavily on opioids, we have progressed to multimodal pathways that consist of various medications (opioids, ketamine, nonsteroidal anti-inflammatory drugs, acetaminophen, etc.) as well as ultrasound-guided nerve blocks (UGNBs). Our center has incorporated UGNBs into our practice for more than a decade to achieve optimal pain control, and most of our clinicians (including residents, physician assistants, and nurse practitioners) have become facile in ED-based blocks for numerous injuries. We have been fortunate to teach numerous clinicians the basics of UGNBs and allow them to develop comfort with the skill set needed for optimal acute pain management.
Explore This Issue
ACEP Now: Vol 38 – No 09 – September 2019This series of articles—starting with the ultrasound-guided femoral nerve block—will discuss common errors that we have seen from our learners. We hope that these minor adjustments in technique will improve UGNB efficacy and spur more clinicians to incorporate these techniques into their armamentarium for optimal pain management.
The goal of the ultrasound-guided femoral nerve block is to offer partial pain control for acute hip fracture (including femoral neck and intertrochanteric fracture). A single injection block performed at the bedside can reduce pain by about 50 percent and decreases IV pain medication requirements. Some data suggest that early ultrasound-guided femoral nerve blocks in patients with hip fractures may improve functional outcomes.1-3
Technique
Classically, the femoral nerve sits just lateral to the femoral artery and is held in close approximation to the Iliac muscle by the fascia iliaca. Placing the ultrasound probe just below the inguinal crease with the probe marker aimed to the patient’s right allows clear visualization of relevant anatomy. The fascia iliaca is the key structure to identify when performing the ultrasound-guided femoral nerve block (see Figures 1 and 2). For a successful ultrasound-guided nerve block, the goal is to place the tip of your needle just under the fascia iliaca. Once in the proper location, injection of anesthetic (or normal saline for hydrodissection) will be clearly seen as black (anechoic) fluid that will spread between the fascial plane and the iliacus muscle. With this technique, the needle stays far away from both the femoral nerve and artery, improving procedural safety (see Figure 3). Also, to prevent exceeding the maximal suggested dosing of anesthetics, we recommend referring to a dosing guide when performing any block (http://highlandultrasound.com/med-guide). To simplify the math, in a patient over 50 kg, you can safely deliver either 20 ml of 0.5% bupivicaine or 1% lidocaine.
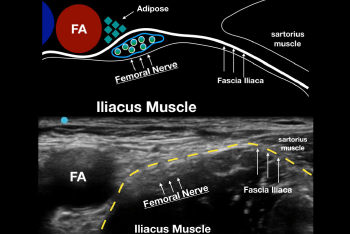
Figure 1: A. Drawing of the relevant sonoanatomy when performing an ultrasound-guided femoral nerve block. Note that the fascia iliaca keeps the femoral nerve right next to the iliacus muscle. B. Ultrasound image of the same anatomy. The fascia iliaca (yellow dotted line) is the key structure to recognize when performing the block.
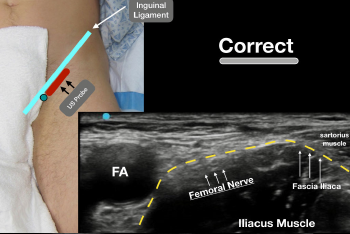
Figure 2: Place the ultrasound probe (with the probe marker facing to the patient’s right/green circle) just under the inguinal ligament so that the relevant anatomy is clearly visualized.
For a more detailed explanation of the procedure, please refer to the previous articles on ultrasound-guided femoral nerve blocks published in ACEP Now (www.acepnow.com/article/ultrasound-guided-femoral-nerve-block).4
In our experience, when novice clinicians are able to locate this classic sonoanatomy, the procedure is often easily performed, leading to low rates of block failure. Unfortunately, we have noticed two common errors when defining the relevant sonoanatomy that can be easily remedied by minor probe manipulations.
Error 1: Probe Placement Distal to Femoral Artery Bifurcation
To obtain the classic sonographic view needed for successful ultrasound-guided femoral nerve block, the clinician must image at the level of the common femoral artery. We have observed that many clinicians place the ultrasound probe distal to the bifurcation of the common femoral artery, imaging the superficial and deep femoral arteries. At this level, the femoral nerve and the fascia iliaca can be difficult to locate. We recommend sliding the probe cephalad and positioning it just below the inguinal ligament so that the common femoral artery is clearly visualized (see Figure 4).
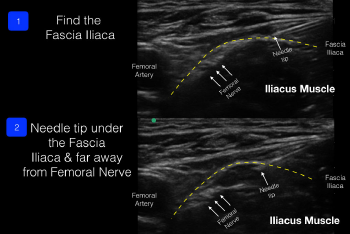
Figure 3: The block needle enters from lateral to medial and deposits anesthetic under the fascia iliaca (away from the femoral nerve and artery).
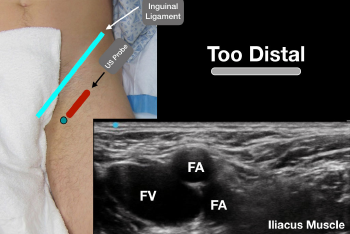
Figure 4: Error 1: The ultrasound probe is too distal in the thigh. The femoral artery has split into the deep and superficial femoral arteries, making visualization of the fascia iliaca and iliacus muscle difficult.
Error 2: Probe at the Wrong Angle in Relation to Femoral Artery
Another error that we commonly see is incorrect probe angle. The ultrasound probe needs to be oriented perpendicular to the common femoral artery to obtain an optimal view of the sonoanatomy. If the probe angle is incorrect, the femoral artery will be visualized, but the clear fascia iliaca and iliacus muscle can be difficult to locate. By keeping the probe parallel to the inguinal ligament, visualization of the femoral artery and nerve bundle will be easily obtained (see Figure 5).
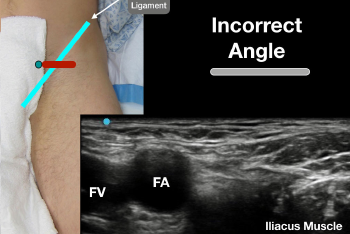
Figure 5: Error 2: The angle of the probe is not perpendicular to the femoral artery, making the fascia iliaca and iliacus muscle difficult to identify.
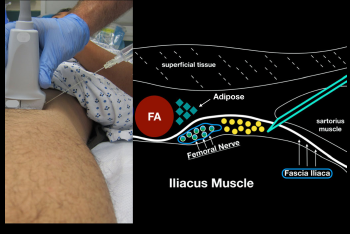
Figure 6: When performing an in-plane lateral to medial approach to the ultrasound-guided femoral nerve block, obtain clear sonoanatomy by proper probe positioning. Try to get your block needle just under the fascia iliaca (lateral to the femoral nerve) and inject anesthetic gently.
Conclusion
The ultrasound-guided femoral nerve block is an ideal single-injection block for emergency clinicians to incorporate into their practice. This technique as part of a multimodal approach to the pain management of the acutely injured patient is supported by literature and can be performed relatively easily at the bedside. Recognizing two common errors in probe placement can help the novice clinician find important sonoanatomy and perform the block with a high degree of confidence and accuracy. Our technique allows for the needle to be far away from the femoral nerve and artery while allowing anesthetic to be deposited under the important fascial plane (the fascia iliaca) (see Figure 6). Offering optimal multimodal pain control for acute injuries by integrating ultrasound-guided femoral nerve blocks is the core responsibility of the practicing emergency physician.
Dr. Nagdev is director of emergency ultrasound at Highland General Hospital, Alameda Health System in Oakland, California.
Dr. Mantuani is director of ultrasound fellowship at Highland General Hospital.
References
- Beaudoin FL, Haran JP, Liebmann O. A comparison of ultrasound-guided three-in-one femoral nerve block versus parenteral opioids alone for analgesia in emergency department patients with hip fractures: a randomized controlled trial. Acad Emerg Med. 2013;20(6):584-591.
- Morrison RS, Dickman E, Hwang U, et al. Regional nerve blocks improve pain and functional outcomes in hip fracture: a randomized controlled trial. J Am Geriatr Soc. 2016;64(12):2433-2439.
- Mouzopoulos G, Vasiliadis G, Lasanianos N, et al. Fascia iliaca block prophylaxis for hip fracture patients at risk for delirium: a randomized placebo-controlled study. J Orthop Traumatol. 2009;10(3):127-133.
- Herring A, Stone MB, Nagdev A, et al. Ultrasound-guided femoral nerve block. ACEP Now. 2011;30(12). Accessed Aug. 15, 2019.




No Responses to “Avoid These Two Common Femoral Nerve-Block Errors”