Figure 2B: Basic position of the ultrasound transducer in the region of the inguinal ligament. The green line (A) indicates the first position. In this position, the femoral head and femoral artery will be located. The blue line (B) indicates a minor adjustment in order to locate the ideal location for the PENG block.[/caption]
Explore This Issue
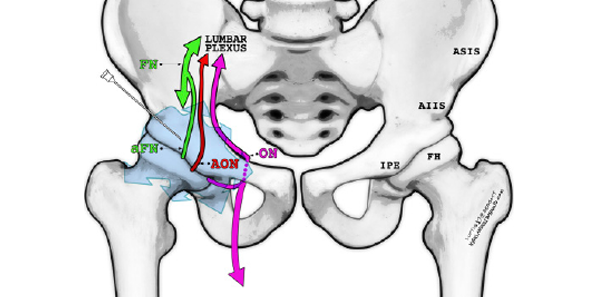
ACEP Now: Vol 41 – No 02 – February 2022Specifically targeting these articular sensory nerves within the myofascial plane of the psoas muscle and ilium can provide superior pain control for hip fractures while also avoiding most of the motor deficits associated with FNB/FIBs. Additionally, anesthetizing the obturator nerve at this level can provide pain control for fractures involving the rest of the pelvis, in particular pelvic rami fractures.9
Supplies
- Low-frequency curvilinear transducer (5-2 MHz) allows for greater visualization of surrounding landmarks. In thin patients and when learning to locate relevant anatomy, we recommend a high-frequency linear transducer (13-6 MHz).
- Anesthetic: approximately 20–30 mL bupivacaine 0.5 percent (5 mg/mL; maximum 2 mg/kg); lower volumes for hip fractures and higher volumes for pelvic fractures. In large-volume plane blocks, always refer to a reputable weight-based local anesthetic (LA) dosing chart such as HighlandUltrasound.com or MDCalc.com.10,11
- Normal saline flushes 10–20 mL. Can be mixed into the same syringe with the LA or injected separately to initially open up the fascial plane (hydrodissection).
- 100-mm 21 g blunt-tip block needle or 20–22 g Quincke spinal needle. Needle visualization for deep target blocks is significantly easier when using echogenic block needles.
- 91-cm or 36-inch tubing.
- Chlorhexidine skin prep.
- Transparent dressing (Tegaderm) for the transducer and sterile gel packets.
- 25–30 g needle for local skin wheal.
Procedure
Pre-block
The patient should be placed on continuous cardiac monitoring and pulse oximetry whenever performing a high-volume ultrasound-guided nerve block. Additionally, the clinician should be knowledgeable of the signs, symptoms, and treatment of local anesthetic systemic toxicity (LAST) and have 20 percent lipid emulsion therapy readily available for this rare but potentially serious complication.12
Positioning
The PENG block is performed with the patient in a supine position. Place the ultrasound system contralateral to the affected hip to allow for clear line of sight. An in-plane lateral to medial approach will allow the operator to visualize the needle tip during the entire procedure (see Figure 2A).
Survey Scan
Place the curvilinear transducer parallel to and over the inguinal crease. Identify the femoral vessels medially and the rounded anterior surface of the femoral head laterally (see Figure 2B). The femoral nerve, which is not targeted in the PENG block, lies just lateral to the femoral artery. While maintaining the same orientation parallel to the inguinal crease, slide the transducer cephalad until the bony ilium is visualized. Also note the anterior inferior iliac spine (AIIS) and iliopubic eminence (IPE) (see Figures 3A and 3B). The rounded hyperechoic psoas tendon (PT) resides along the ilium between these two structures. The target of the PENG block is the fascial plane over the ilium just lateral and deep to the psoas tendon. Note that the femoral vessels and nerve are both medial and far from the needle pathway.
Pages: 1 2 3 4 5 | Single Page




No Responses to “Benefits of Using the Pericapsular Nerve Group (PENG) Block”