Explore This Issue
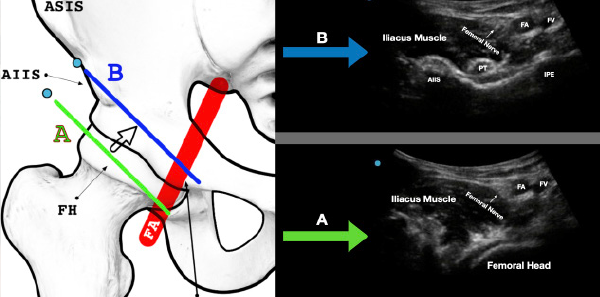
ACEP Now: Vol 41 – No 02 – February 2022Figure 3A: The green line (A) indicates the initial location. Note the femoral artery (FA) and femoral vein (FV) as well as the femoral head.
Figure 3B: Maintaining the probe parallel to the inguinal crease, slide the probe a bit cephalad. The blue line (B) indicates the ideal location for the PENG block. Note the anterior inferior iliac spine (AIIS), the iliopubic eminence (IPE), and the psoas tendon (PT). The femoral vasculature (FA/FV) and femoral nerve in the proximal aspect of the ultrasound screen will often be visible at this location.
Skin Wheal
After satisfactory identification of the landmarks noted on the survey scan, widely prep the skin with chlorhexidine. Allow this to completely dry and place 2–3 mL lidocaine skin wheal 2–3 cm lateral to the transducer.
Needle Entry
Using a lateral to medial in-plane approach, advance the block needle at a 30 degree to 45 degree angle toward the bony ilium just deep and lateral to the psoas tendon. After the first 1–2 cm, the angle may be slightly redirected to reach this target. With deep blocks that require steep trajectories such as the PENG block, needle visualization may be difficult. “Toeing in” the transducer so that the ultrasound beam is more parallel to the needle can improve visualization.13 Continue advancing the needle until it reaches the hard bony backstop of the ilium. After aspiration, gently hydrodissect this overlaying fascial plane. Proper needle placement will demonstrate anechoic fluid of LA injected underneath the psoas tendon, lifting it upward and spreading medially. If resistance is encountered during injection or fluid is not visualized entering the fascial plane, this can be corrected by slightly rotating the needle and reattempting injection until proper spread is visualized. This needle rotation repositions the needle-tip bevel and assists with penetration into the fascial plane. Once satisfied with the needle placement, slowly inject the remainder of the 20–30 mL of local anesthetic into the already-open fascial plane (see Figures 4 and 5).
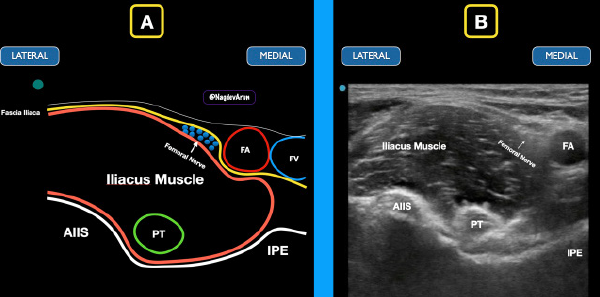
Figure 4: Schematic drawing (A) and ultrasound image (B) of the classic location of the PENG block. Note the fascia iliaca in relation to the femoral nerve, femoral artery (FA), and femoral vein (FV). Note the anterior inferior iliac spine (AIIS), iliopubic eminence (IPE), and psoas tendon (PT).
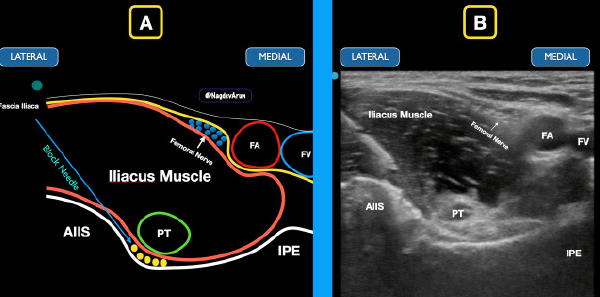
Figure 5: The block needle comes from a lateral to medial approach to deposit anesthetic under the iliacus muscle. The goal is to spread anechoic anesthetic (yellow circles) under the psoas tendon between the iliacus muscle and the bony ramus.
Pages: 1 2 3 4 5 | Single Page




No Responses to “Benefits of Using the Pericapsular Nerve Group (PENG) Block”