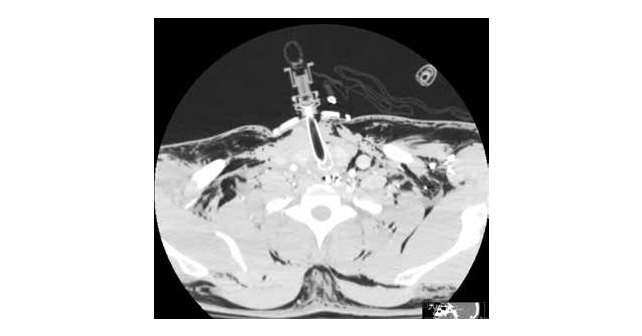
A 34-year-old male was involved in a motorcycle rollover. His vehicle hit a pole, and he was hit in the throat with the handlebars of his bike. He presents alert and awake, with gross facial and neck swelling, and no history of loss of consciousness. His Glasgow Coma Scale is 15. Notable on his physical examination is subcutaneous emphysema diffusely, including crepitus to palpation of radial pulses, and crepitus in his face, neck, torso, and scrotum. X-ray confirms subcutaneous emphysema (see Figure 1). There are no external lacerations.
Explore This Issue
ACEP Now: Vol 42 – No 04 – April 2023
FIGURE 1: Initial chest X-ray taken supine demonstrating massive subcutaneous emphysema. Of note: Bilateral pneumothoraces are visible on the chest CT (See Figure 2) but are not clear on the initial chest X-ray. He received chest tubes thereafter.
To protect his airway, an awake intubation is planned. He is administered nebulized lidocaine and ketamine. He develops severe respiratory distress and becomes unable to phonate. Intubation with a Glidescope is unsuccessful, and he is biting the tube.
The surgery team performed an emergency surgical airway.
The surgical procedure note read as follows: “His midline had been marked. Incision with a 10 blade was made over this line. The scalpel was used to divide the subcutaneous tissue, which was bleeding profusely. Then I suddenly encountered massive spewing of dark red non-pulsatile blood into the field.
“With suctioning, gauze packing, and retractors, I was able to somewhat control the bleeding, and I used my finger to explore the wound. I felt the laryngeal prominence and traced this down to a boggy area that I hoped was the cricoid membrane. There were crunchy things in the area which I assumed were shattered pieces of cartilage. I used a hemostat to bluntly poke a hole into the boggy area and spread to dilate the hole. I used my finger to explore the hole and initially felt the inside of the larynx, so I knew I was in the airway.
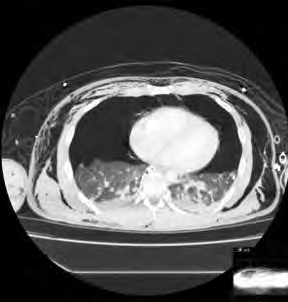
FIGURE 2: CT chest demonstrating large bilateral pneumothorax and subcutaneous emphysema. Laryngeal-tracheal separation may occur. Insertion of an endotracheal tube may cause separation of the trachea from the larynx, if the connection is tenuous. A transected cervical trachea may retract into the mediastinum and have to be surgically retrieved/extracted to establish an airway.
“At a very sharp angle inferiorly, I was able to feel tracheal rings. I passed a pediatric bougie into the trachea and then over this slid a 6-0 cuffed endotracheal tube (ETT) into the airway. One of my colleagues blew up the balloon and began ventilating the patient. The endotracheal tube is sutured to the skin of the anterior neck with 0 silk. End-tidal CO2 confirms placement in the trachea.”
Pages: 1 2 3 4 | Single Page




No Responses to “Case Report: Blunt Tracheal Injury Creates Difficult Airway”