How Difficult Airways Present
The American Society of Anesthesiologists’ practice guidelines define a difficult airway as a clinical situation in which a conventionally trained anesthesiologist experiences difficulty with facemask ventilation of the upper airway, difficulty with tracheal intubation, or both. Difficult laryngoscopy is defined as inability to visualize any portion of the vocal cords after multiple attempts. Difficult tracheal intubation entails multiple attempts at intubation, in the presence or absence of tracheal pathology.1
Explore This Issue
ACEP Now: Vol 42 – No 04 – April 2023
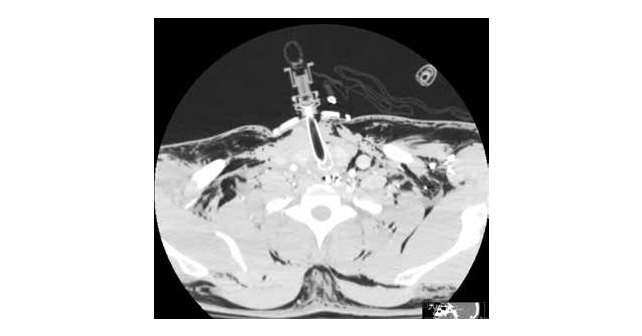
FIGURE 3: CT demonstrating T-tube in airway, at approximately the C3-4 level, along with air diffusely in soft tissue. An important takeaway is that if the tracheostomy tube is dislodged, the patient cannot be intubated from above. The neck must be re-explored to establish an airway. The author does not in general recommend CT to confirm airway placement. In fact, there was positive end tidal CO2 after the 6-0 cuffed ETT was sutured into the patient’s airway.
There are many non-traumatic disease states which may contribute: ankylosis, degenerative osteoarthritis, subglottic stenosis, lingual thyroid, tonsillar hypertrophy, or congenital nontraumatic abnormalities such as Down syndrome, Pierre Robin, and Treacher-Collins. For purposes of this discussion, we will concentrate on traumatic injury.
Tracheobronchial injury occurs in an estimated 10 to 20 percent of patients with penetrating trauma to the neck.2 In a retrospective review of 12,187 patients treated at a civilian trauma center in Toronto over 16 years, 36 patients (0.3 percent) suffered blunt airway injury.3 Blunt trauma to the neck may be more complicated. Of course, in these cases, intubation directly through the wound is not an option. Over recent decades, the availability of video-laryngoscopy (VL) and fiberoptic intubation/ bronchoscopy (FOB) have reduced both the rate of failed intubation and the need to perform emergency surgical airways.
Another report enumerating over 12,000 trauma cases over a seven-year period listed 242 patients requiring a surgical airway. When only the 3,271 patients with trauma to the head and neck were considered, a mere 51 cases required a surgical airway, and of these, 47 cases made it to the operating room for a surgical tracheostomy.4 Since traumatic airway injury is rare, assessment and management are not well characterized. Trauma may also entail a variety of contributing factors. For example, retropharyngeal hematomas have been reported following cervical spine injury, foreign body ingestion, central line placement, and coagulation disorders.5,6
Other measures may help, although they were of limited value in the above case. Opportunities for supplemental oxygen include oxygen delivery by nasal cannula, facemask or laryngeal-mask airway, and blow-by. Clearly, in the case above, these measures were temporizing at best. In fact, the patient’s arterial blood gas just prior to surgical intervention revealed a pH of 7.105, pCO2=87, and pO2=62.
Pages: 1 2 3 4 | Single Page




No Responses to “Case Report: Blunt Tracheal Injury Creates Difficult Airway”