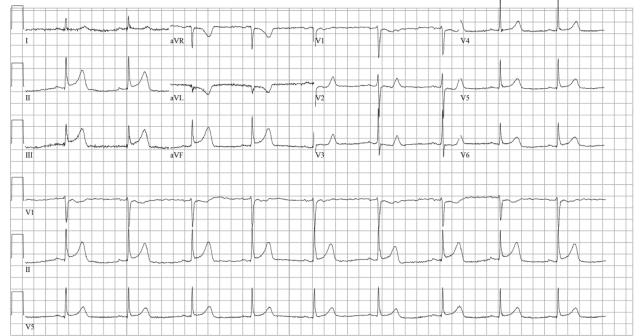
Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. The ECG showed ST-segment elevation without obstructive coronary disease. Coronary vasospasm is linked to either hyperreactivity or vasoconstrictor stimuli on vascular smooth muscle cells. Vasodilators, like nitrates and calcium channel antagonists, are standard treatments.4
Explore This Issue
ACEP Now: Vol 43 – No 12 – December 2024Amphetamines are central nervous system stimulants that release catecholamines, creating a hyperadrenergic state.5 Developed more than 100 years ago, its illicit use has surged in the last 25 years. Methamphetamine can cause severe cardiovascular effects, including elevated blood pressure, vasospasm, and atherosclerotic disease. The mechanisms in methamphetamine users are not well understood. Acute exposure promotes vasoconstriction and cerebral hypoperfusion due to neurovascular damage and imbalance of vasoregulatory substances.6 Vascular tone and blood pressure are regulated by neuronal stimulation and endothelial-derived substances.7 Endothelin, angiotensin II, and catecholamines cause vasoconstriction via G protein-coupled receptors, whereas vasodilators like nitric oxide reduce contraction by inhibiting calcium influx or myosin phosphorylation. Methamphetamine-induced vasoconstriction involves endothelial release of endothelin-1 or arterial TAAR1 signaling. Methamphetamine use is often associated with acute angina and coronary vasospasm, reducing blood flow to cardiac tissue.
We present a case of refractory ventricular fibrillation resuscitation due to coronary vasospasm from recent amphetamine use with IV NTG. No existing algorithm or literature guides the validity of a NTG strategy for vasospastic cardiac arrest in the emergency department. We hypothesize that OHCA in younger patients could often be attributed to coronary vasospasm and that traditional ACLS strategies may exacerbate the condition. Further studies are needed to develop safe resuscitation strategies for these patients.
 Dr. Godwin is a recent graduate from the Kennestone Emergency Medicine Residency Program and currently works as an emergency physician at Atrium Health Floyd in Rome, Ga.
Dr. Godwin is a recent graduate from the Kennestone Emergency Medicine Residency Program and currently works as an emergency physician at Atrium Health Floyd in Rome, Ga.
 Dr. Accilian is an emergency physician at Wellstar Kennestone Regional Medical Center, Marietta, Ga.
Dr. Accilian is an emergency physician at Wellstar Kennestone Regional Medical Center, Marietta, Ga.
 Dr. Rad is ED faculty at Wellstar Kennestone Regional Medical Center in Marietta, Ga., and at Naples Community Hospital in Naples, Fla.
Dr. Rad is ED faculty at Wellstar Kennestone Regional Medical Center in Marietta, Ga., and at Naples Community Hospital in Naples, Fla.
References
- Prinzmetal M, Kennamer R, Merliss R, et al. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959;27:375-388.
- Myerburg RJ, Kessler KM, Mallon SM et al. Life-threatening ventricular arrhythmias in patients with silent myocardial ischemia due to coronary-artery spasm. N Engl J Med. 1992;326(22):1451-1455.
- Magid DJ, Aziz K, Cheng A, et al. Part 2: evidence evaluation and guidelines development: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16 suppl_2):S358–S365.
- Lanza GA, Careri G, Crea F. Mechanisms of coronary artery spasm. Circulation. 2011;124(16):1774-1782.
- Yamamoto BK, Moszczynska A, Gudelsky GA. Amphetamine toxicities: classical and emerging mechanisms. Ann N Y Acad Sci. 2010;1187:101-121.
- Kousik SM, Graves SM, Napier TC, et al. Methamphetamine-induced vascular changes lead to striatal hypoxia and dopamine reduction. Neuroreport. 2011;22(17):923-928.
- Loh YC, Tan CS, Ch’ng YS, et al. Overview of the microenvironment of vasculature in vascular tone regulation. Int J Mol Sci. 2018;19(1):120.
Pages: 1 2 3 | Single Page



No Responses to “Case Report: Coronary Vasospasm-Induced Cardiac Arrest”