Case
Explore This Issue
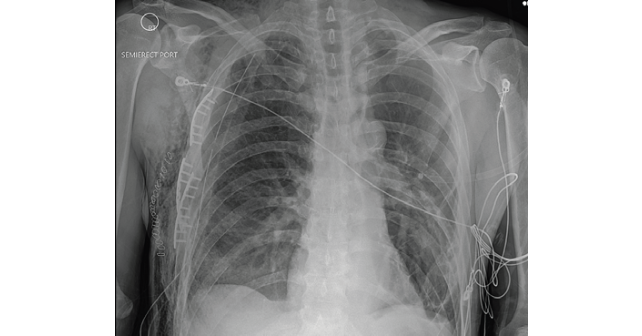
ACEP Now: Vol 42 – No 05 – May 2023FIGURE 1: Chest X-ray of multiple rib fractures (arrows). (Click to enlarge.)
A 58-year-old male with a history of alcohol abuse presented to the emergency department (ED) as a category 2 trauma for a fall with a reported flail chest. The patient had been drinking with friends when he was witnessed to trip and fall a distance of one step. His right chest wall struck a protuberance, initially reported to be the edge of a stair and later noted to be tree stump. EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest. The splint consisted of a folded blanket placed over the mobile segment and held in place with tape. The patient complained of right chest wall pain and shortness of breath that improved once splinted. He denied syncope, head trauma, or any other complaints. His vital signs were within normal limits except for a respiratory rate of 23 with a room air pulse oxygen in the upper 90s. Exam was notable for bilateral breath sounds though diminished on the right, with a mobile segment on the right lateral chest wall. The patient experienced significantly more discomfort with the splint removed and it was reapplied during his trauma bay evaluation. There were no open wounds and the remainder of his exam was unremarkable.

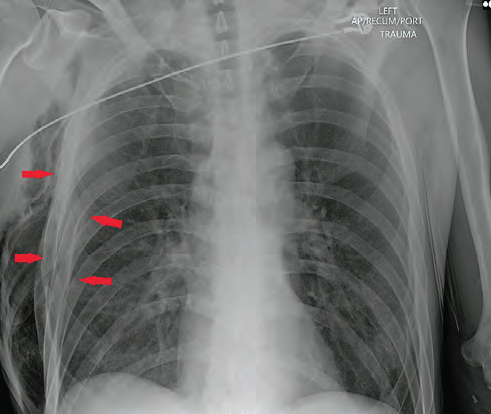
FIGURE 2: Axial chest CT of the chest wall defect (red arrow) and pneumothorax trauma (white arrows). (Click to enlarge.)
Trauma imaging was performed including bedside X-rays of the chest and pelvis. The chest X-ray showed multiple displaced right rib fractures and chest wall subcutaneous emphysema without definitive evidence of a pneumothorax, as well as right lower lobe atelectasis versus contusion (Figure 1). The patient was placed on oxygen for his dyspnea, administered pain medication, and was taken for computed tomography (CT). CTs of his head, spine, chest, abdomen, and pelvis were performed. A chest CT demonstrated multiple displaced right lateral rib fractures with direct communication between the pleural space and the soft tissue. There was evidence of a decompressed pneumothorax into the soft tissues of the right lateral chest wall with evidence of developing tension within the soft tissues. Extensive subcutaneous emphysema was dissecting from the chest disruption superiorly into the neck and inferiorly into the lower chest and abdominal wall (Figures 2 and 3).
Pages: 1 2 3 | Single Page




No Responses to “Case Report: EMS Says Flail Chest, But Is It?”