
Explore This Issue
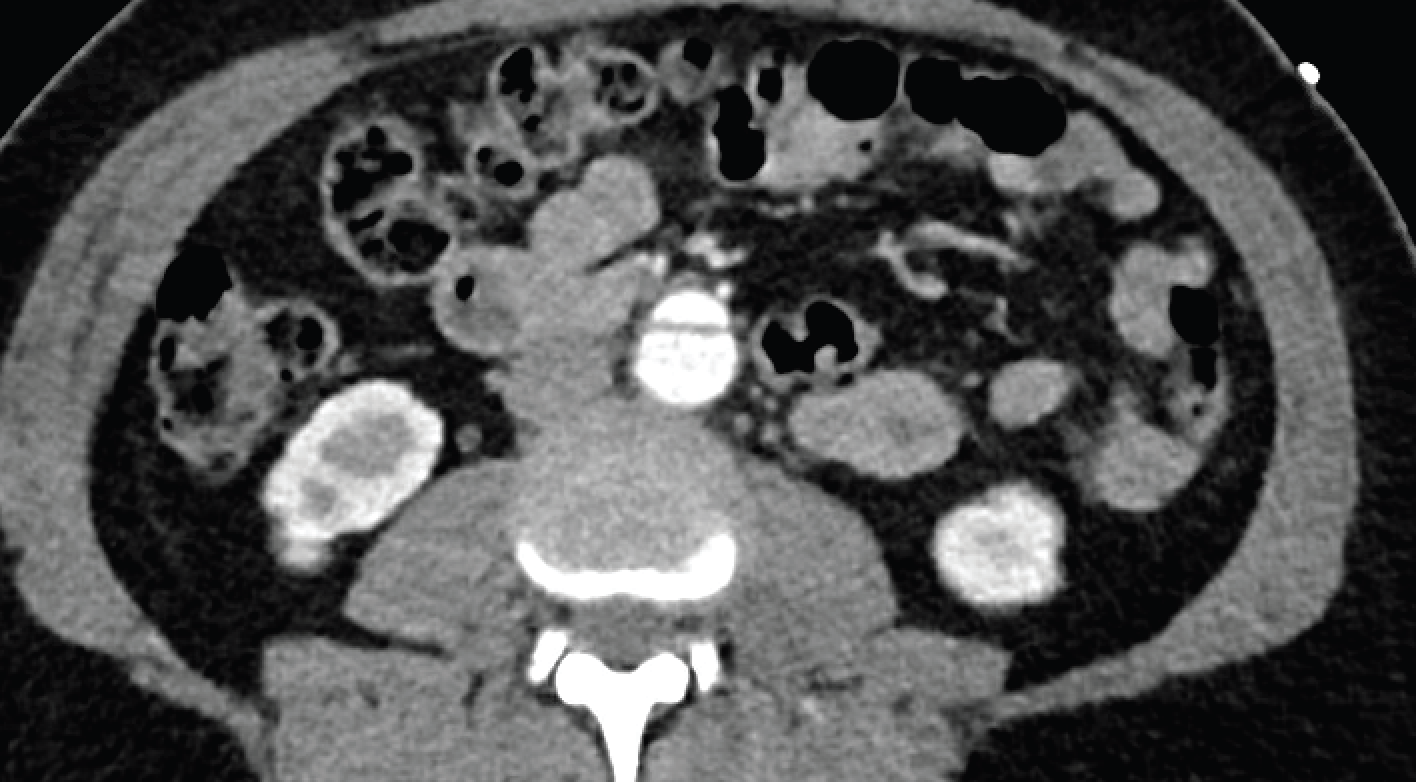
ACEP Now: Vol 43 – No 07 – July 2024Axial abdominal aortic dissection. (Click to enlarge.)
Treatment of the stable patient with TAI begins with blood pressure and heart rate stabilization, with pharmacologic management reducing risk of aortic rupture to less than two percent.3 Esmolol is the preferred medication for stabilization of aortic dissection and aortic aneurysm due to its pharmacokinetics and wide availability. Diltiazem, nicardipine, and nitroprusside should be considered as adjuncts.3 Of note, administration of nitroprussides before beta blockers can propagate aortic dissection due to the reflex catecholaminergic surge secondary to vasodilation, resulting in increased inotropy and downstream shearing forces on the aorta.4 To date, there are few evidence-based criteria for specific blood pressure goals in aortic dissection—ranging anywhere from 100 mmHg-140 mmHg systolic—although it has been shown that systolic blood pressure below 70 mmHg increases mortality.4 Meanwhile, guidelines for heart rate are more concrete, supporting optimization below 100 bpm, ideally 50-60 bpm.3,4
The cutoff for necessity of operative intervention beyond medical management is primarily determined by the grade of aortic injury as determined by CT angiography.3 Grade I involves intimal tear, Grade II involves intramural hematoma, Grade III is a pseudoaneurysm, and Grade IV is considered rupture; injuries rated Grade II and above are eligible for operative intervention.3 Morbidity, mortality, and risk of reintervention are decreased by medically temporizing patients for surgical intervention outside of the high-risk window: 24 hours of onset until two weeks from injury.1,3 Temporizing measures are not always possible for critically ill Grade IV patients, and outcomes are usually much worse.3 Fortunately, this case was found to be an uncomplicated Grade III dissection, which was determined to be safe for delayed endografting.
The patient stayed a total of nine days in the hospital and was discharged with a stable aortic dissection planned for future endovascular repair. Her orthopedic injury was managed non-operatively until her aortic repair could be performed.
 Dr. Arnot is a PGY-1 at the University of Arizona department of emergency medicine.
Dr. Arnot is a PGY-1 at the University of Arizona department of emergency medicine.
 Dr. Denq is an emergency physician at the University of Arizona department of emergency medicine.
Dr. Denq is an emergency physician at the University of Arizona department of emergency medicine.
References
- Huu AL, Olive JK, Cekmeceliouglu D, et al. Endovascular therapy for patients with heritable thoracic aortic disease. Ann Cardiothorac Surg. 2022;11(1):31-36.
- Mazzaccaro D, Righini P, Fancoli F, et al. Blunt thoracic aortic injury. J Clin Med. 2023;12(8):2903. Published 2023 Apr 17.
- Mouawad NJ, Paulisin J, Hofmeister S, et al. Blunt thoracic aortic injury–concepts and management. J Cardiothorac Surg. 2020;15(1):62.
- Sayed A, Munir M, Bahbah EI. Aortic Dissection: A Review of the Pathophysiology, Management and Prospective Advances. Curr Cardiol Rev. 2021;17(4):e230421186875.
Pages: 1 2 3 | Single Page




No Responses to “Case Report: Imaging Follows Dangerous ATV Accident”