
A 27-year-old female patient presents to the emergency department (ED) with a chief complaint of fatigue and shortness of breath over the last two weeks.
Explore This Issue
ACEP Now: Jan 01She reports generally low energy levels over the past month. She developed mild dyspnea on exertion two weeks ago. She felt short of breath simply trying to get out of bed this morning, and this prompted her to seek evaluation.
The patient has otherwise been healthy and reports no significant past medical history. Her social history is unrevealing. She denies having a family history of heart disease. When asked about current or recent pregnancy, the patient states that she delivered a healthy, full-term baby four months ago, preceded by an uncomplicated pregnancy.
On exam, the patient generally appears well.
Vital signs:
- Temperature 37.1 °C
- Heart rate 101
- Respiratory rate 28
- Blood pressure 130/76
- Oxygen saturation 90 percent
Her physical examination is notable for stage 2+ pitting edema of the bilateral lower extremities, and the presence of bibasilar crackles on auscultation of the lungs. No abnormal cardiac sounds are appreciated. Her abdomen is soft, nontender, and nondistended. Prominent jugular veins are appreciated.
Differential Diagnosis
The differential diagnosis on this patient includes myocardial infarction, congestive heart failure, myocarditis, pericarditis, pulmonary embolism, pneumonia, pleural effusion, pulmonary edema, anemia, hypothyroidism, cardiac arrhythmia, aortic dissection, and peripartum cardiomyopathy.
Workup
The evaluation of this patient’s chief complaint includes a 12-lead ECG and a chest radiograph. Laboratory tests including troponin, brain natriuretic peptide (BNP), complete blood count, electrolyte panel, and a pregnancy test should be obtained. Point-of-care bedside echo may be helpful to evaluate the global systolic function of the left ventricle, to assess for significant right ventricular enlargement, and to evaluate for the presence of a pericardial effusion. Point-of-care ultrasound of the lungs may reveal the presence of B-lines, which would be concerning for pulmonary edema in this patient. Pleural effusions are also typically apparent on lung ultrasonography.
Ambulatory pulse oximetry test may unmask worsening hypoxia in the setting of physical activity.
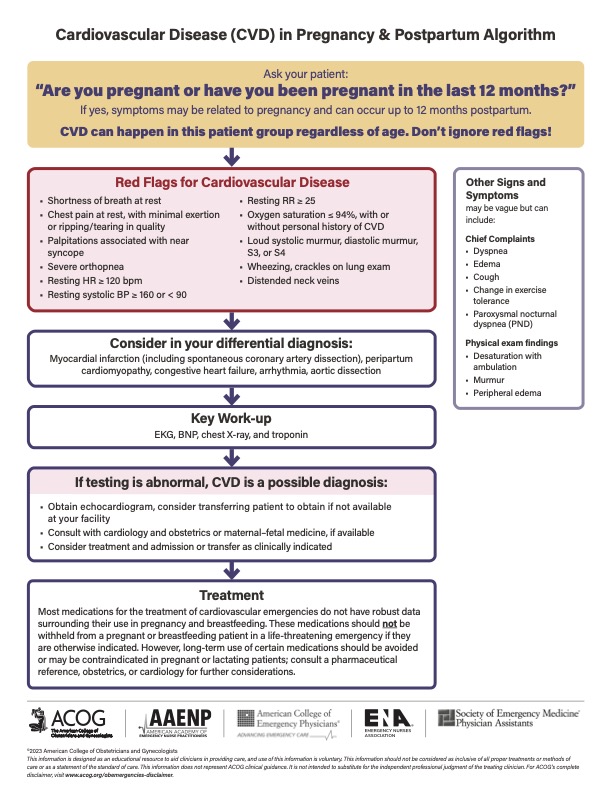
Click to enlarge the algorithm.
Management
Pregnancy-related cardiovascular disease is a rare but serious complication of pregnancy and accounts for a significant proportion of maternal morbidity and mortality. Cardiovascular disease is the second most common cause of pregnancy-related death in the United States, and is the leading cause of pregnancy-related death among non-Hispanic Black patients.1 Cardiovascular disease during or after pregnancy—collectively representing an array of conditions involving disease and dysfunction of the heart and vascular system—encompasses the diagnoses of myocardial infarction (including spontaneous coronary artery dissection), cardiac arrhythmia, congestive heart failure, aortic dissection, and peripartum cardiomyopathy.
Pages: 1 2 3 | Single Page




No Responses to “Peripartum Cardiovascular Disease Is Rare, But Serious”