The Case
A 69-year-old male presents to the emergency department for evaluation of diplopia. Three days prior, he had developed left-sided periorbital and ocular aching pain. He then noticed decreased peripheral vision on the left. The patient denies worsening pain with extraocular muscle movement. He also denies photosensitivity, eye redness, discharge, flashing lights, floaters, or a curtain or veil over his vision. He hasn’t experienced headache, temple pain, jaw claudication, or fever, and there are no other neurological symptoms, such as extremity numbness, weakness, or slurred speech. He denies any recent trauma.
Explore This Issue
ACEP Now: Vol 37 – No 12 – December 2018On physical examination, he is afebrile, and his vital signs are within normal limits. His ocular exam is notable for the following:
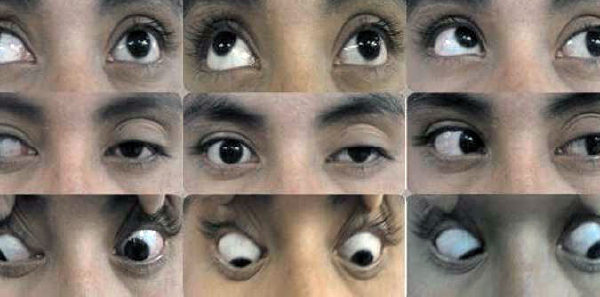
- Left eye: ptosis, weak adduction, no abduction
- Pupils: 3 mm bilaterally and reactive to light
- Visual acuity: right eye 20/30, left eye 20/25, no afferent pupillary defect
The remainder of his examination is normal.
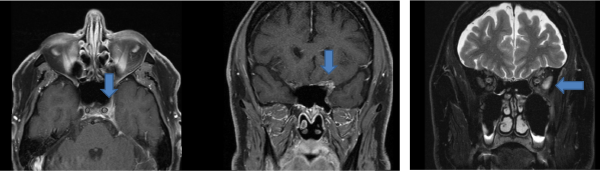
The patient undergoes an MRI of the brain and orbits, which reveals an increased T2 signal with enhancement involving the left lateral rectus muscle and intraconal fat (orbital compartment) extending into the orbital apex and left cavernous sinus.
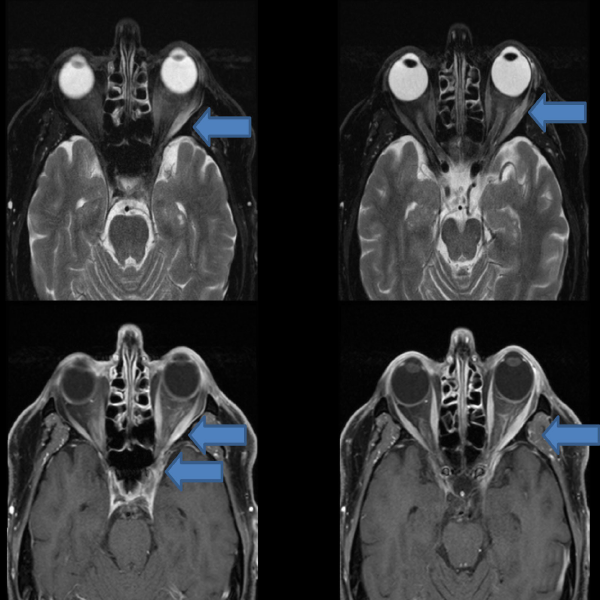
The patient’s MRI revealed an increased T2 signal with abnormal enhancement within the left lateral rectus muscle and intraconal fat extending into the orbital apex and left cavernous sinus.
Ethan Sterk
He is admitted to the neurology service, and subsequent workup includes the following tests: erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody, antineutrophil cytoplasmic antibody, rapid plasma reagin, double-stranded DNA antibody, Lyme polymerase chain reaction, angiotensin-converting enzyme (ACE), and anti-smooth muscle antibody. They are all negative. Also, cerebrospinal fluid (CSF) testing is remarkable for a glucose of 99, a protein of 93, and one white blood cell. CSF cultures are negative; ACE and Lyme antibodies are also negative. Ophthalmology is consulted, and the patient is diagnosed with Tolosa-Hunt syndrome.
Discussion
Tolosa-Hunt syndrome is rare, with an estimated incidence of one case per million per year. It is characterized by painful ophthalmoplegia and is caused by an idiopathic granulomatous inflammation of the cavernous sinus. The inflammation produces pressure and secondary dysfunction of the structures within the cavernous sinus, including cranial nerves III, IV, and VI, as well as the superior divisions of cranial nerve V.1–5 Diplopia results from cranial mono- or polyneuropathy. Patients may present at any age. Men and women are affected at the same frequency.4
Pages: 1 2 3 | Single Page




No Responses to “Case Report Provides Tips for Diagnosing the Rare Tolosa-Hunt Syndrome”