Explore This Issue
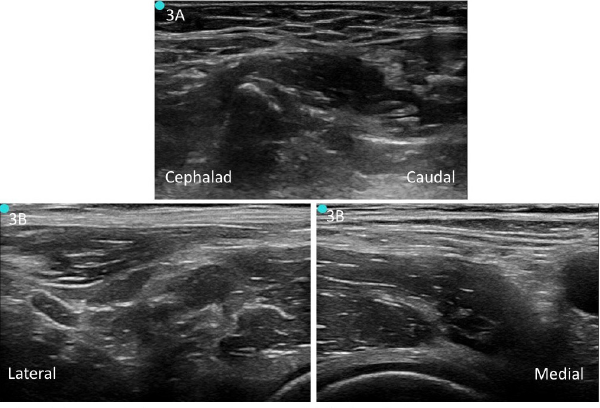
ACEP Now: Vol 37 – No 01 – January 2018Figure 3. A: Unlabeled preprocedure scan of infrainguinal approach. B: Unlabeled preprocedure scan of suprainguinal approach.
To perform a USGFICB, place the patient supine (slight Trendelenburg position if tolerated) and place the US system contralateral to the extremity being blocked. This will allow the clinician to have a clear view of the US screen when performing the block. Perform a preprocedure scan of the anatomy with a linear transducer (6–10MHz) (see Figures 3A and 3B). If aberrant anatomy distorts landmarks and the proper fascial layers cannot be properly identified, consider aborting the procedure. Clean the target needle entry site and probe and make a small skin wheal with 1–2% lidocaine. Clean the area with a chlorhexidine scrub.
Nerve Block Procedures
Infrainguinal USGFICB. Place your US transducer perpendicular to the inguinal ligament at a third of the distance between the anterior superior iliac spine and pubic symphysis (see Figure 4A), with the transducer indicator oriented cephalad. After visualizing the pulsating femoral artery, locate the hyperechoic femoral nerve immediately lateral. Slide the transducer laterally to identify the sartorius muscle caudad and iliacus muscle cephalad, with the fascia lata and fascia iliaca forming a “bow tie” over the iliacus muscle. Place a skin wheal just caudal to the transducer, marking the location that the block needle will enter.
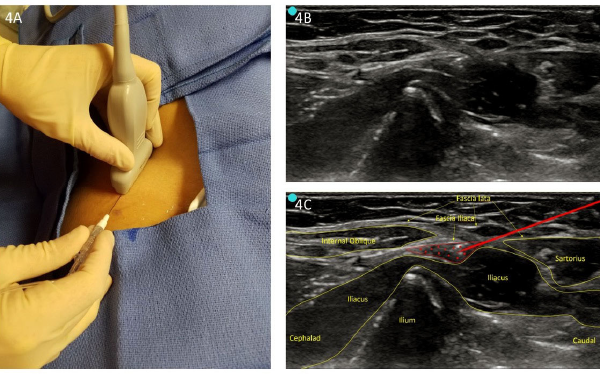
Figure 4. A: Infrainguinal approach (perpendicular to inguinal ligament). B: Unlabeled infrainguinal preprocedure scan. C: Labeled image with infiltration.
Insert the needle in-plane to provide a long view of the needle. Guide the needle below the inguinal ligament and through the fascia lata and fascia iliaca at the center of the “bow tie.” When using a blunt-tipped needle, a palpable “pop” may be felt when puncturing these two fascial layers. Once through the fascia iliaca, aspirate and then inject 2–3 mL of local anesthetic to confirm needle placement (see Figures 4B and 4C). Hydro-dissection of the fascia iliaca from the iliacus muscle demonstrates correct placement. Gently continue to hydro-dissect with 30–60 mL of local anesthetic in 5 mL increments with gentle aspirations between injections to ensure avoidance of inadvertent vascular puncture.
Suprainguinal USGFICB. Place the transducer just superior and parallel to the inguinal ligament (see Figure 5A). Slide the transducer medially to visualize common sonoanatomy (eg, femoral vein, femoral artery, and femoral nerve). Slowly move the transducer laterally to visualize the sartorius muscle overlying the iliacus muscle. Place a skin wheal just lateral to the transducer, marking the location that the block needle will enter. Insert the needle in-plane from lateral to medial, visualizing the needle in long axis. The needle should course through the sartorius muscle or just superficial and sit between the iliacus muscle and fascia iliaca, lateral to the neurovascular bundle.15 Once deep to the fascia iliaca, aspirate and inject 2–3 mL of local anesthetic to confirm needle placement (see Figures 5B and 5C). If there is separation between the fascia iliaca and iliacus muscle, gently hydro-dissect with 30–60 mL of local anesthetic in 5 mlL increments with gentle aspirations between injections to ensure lack of inadvertent vascular puncture.
Pages: 1 2 3 4 | Single Page




5 Responses to “Control Hip Fracture Pain Without Opioids Using Ultrasound-Guided Fascia Iliaca Compartment Block”
January 27, 2018
Ron BraceThe diagram, first color coded one showing locations of Fem nerve vein and artery is seriously mislabeled and a correction need be done; Femoral Vein is in wrong place, as is the Femoral artery – and the fem artery is mislabeled
I am sure by now a thousand people have written about it!
https://www.acepnow.com/wp-content/uploads/2018/01/ACEP_0118_pg20a.png
January 28, 2018
Robert A.Great article. I think Figure 1 is mislabeled: Femoral artery is mislabeled as “Fem V.” and Femoral vein mislabeled as “Fem N. (red)”.
February 5, 2018
HosamIn illustration, I think that order of structures are not proper.it is vien artery nerve from medial to lateral
February 5, 2018
MikeHi, picture 1 seems to have some errors. There are two structures markes Fem N, one of them in red which is likely supposed to be the Fem Artery. If that structure is supposed to the fem artery it is incorrectly positioned medial to the femoral vein when it should be lateral
February 5, 2018
Dawn Antoline-WangThank you to everyone who pointed out the error in Figure 1. The image has been corrected.