Traditional landmarked-based wrist aspirations are difficult and often unsuccessful. Even in the hands of experienced rheumatologists who perform frequent radiocarpal aspirations and injections, landmark-based aspirations in joints throughout the body can be missed more than 60 percent of the time.1
Fortunately, for emergency physicians, the use of point-of-care ultrasound for anatomical visualization allows for easy detection and localization of wrist effusions and for reliable joint aspiration.2 Ultrasound not only makes this procedure easier to perform but should decrease the likelihood of iatrogenic tendon injury.
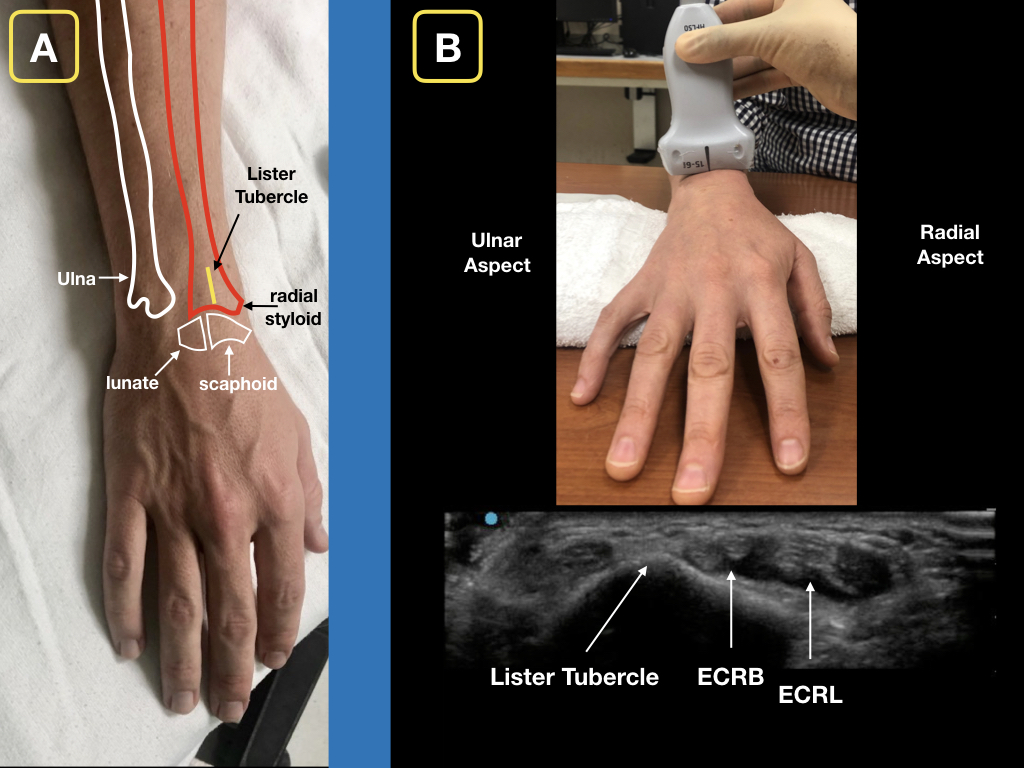
Figure 1A: The dorsal aspect of the distal forearm and radiocarpal joint. Note Lister’s tubercle and its relation to the scaphoid bone. Figure 1B: A roll is placed on the palmar aspect of the wrist for slight flexion. With the ultrasound probe in a transverse orientation, slide distally until Lister’s tubercle is visualized. The extensor carpi radialis brevis tendon (ECRB) and extensor carpi radialis longus (ECRL) can be seen on the radial aspect of Lister’s tubercle. Credit: Arun Nagdev
The radiocarpal joint is composed primarily of the distal radius as it articulates with the scaphoid and lunate bones (see Figure 1A). This can be palpated on the unaffected side but can be difficult to identify by landmarks in many patients, especially with a marked swelling from an inflammatory or infectious process.
Our technique provides an easy-to-obtain ultrasonographic view and reliable method to evaluate the radiocarpal joint and perform an aspiration if needed. We have successfully used this method to rule in and rule out septic arthritis in multiple cases, allowing our clinicians to develop a standard go-to method to assess the radiocarpal joint.
Our Technique
- Begin by scanning the unaffected wrist to visualize normal anatomy. The hand should be pronated. Support the wrist on a flat surface in slight flexion using a towel roll. Using a high-frequency (15–6 MHz) linear transducer in the transverse plane, begin in the distal one-third of the forearm and scan distally to identify the second compartment of the extensor tendons of the wrist. Use Lister’s tubercle as the landmark for the most ulnar aspect of the second compartment, which is composed of the extensor carpi radialis brevis and extensor carpi radialis longus tendons (see Figure 1B). Rotate the transducer to the longitudinal orientation (ie, with the probe marker facing the fingertips), and slide the transducer in a distal manner over the radius and carpus in line with the middle finger, allowing you to visualize the distal radius and the scaphoid. Scan toward the thumb to visualize the entire distal radius. There should be minimal hypoechoic (dark) signal in the radiocarpal space. Also note the overlying extensor tendons (see Figure 2).
Pages: 1 2 3 | Single Page



No Responses to “Easy Ultrasound Technique to Evaluate and Aspirate an Atraumatic Painful Wrist”