Written from the perspective of an emergency physician who also runs a weekly minor fracture clinic, this column will highlight a few key teaching points for commonly missed and commonly mismanaged ED orthopedic cases. This debut column will deal with pediatric distal radius fractures.
Explore This Issue
ACEP Now: Vol 36 – No 10 – October 2017The Cases
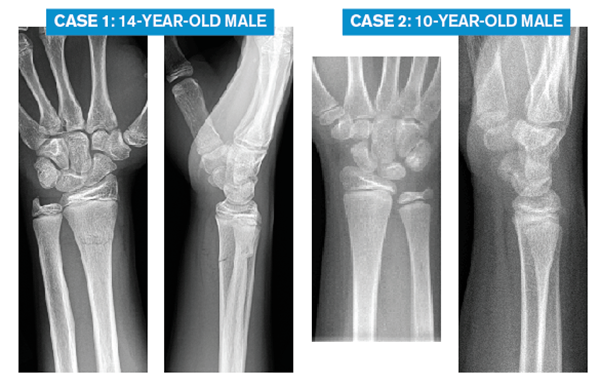
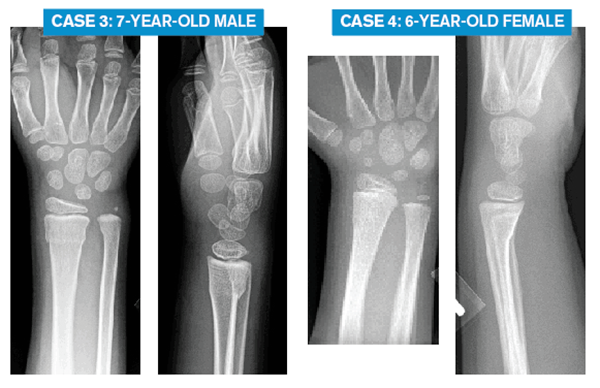
Here are X-rays of four pediatric patients with isolated wrist injuries after a fall. Each is mildly swollen and tender at the distal radius, closed, neurovascularly intact, and without scaphoid (or other carpal) tenderness.
What is your diagnosis, emergency department treatment, and follow-up plan for each?
The Challenge
Of the above four cases, the radiology report for each may read, “buckle fracture of the distal radius.” One case is a simple buckle fracture, and it tends to be overtreated in the emergency department. For the other three cases, they require well-molded immobilization in the emergency department. However, two of the cases should be molded in flexion; the third case, in extension. Optimal ED management requires us to recognize the subtle differences between these pediatric distal radius fractures.
The Clinical Pearls: Pediatric Distal Radius Fractures
- Simple dorsal buckle fractures are stable. Treat for comfort and protection. Removable splints are fine.
- Transverse fractures (also called complete or bicortical fractures) can be subtle on X-ray. If the dorsal buckle fracture extends to the volar side or if the distal fragment is dorsally angulated, then it is not a simple dorsal buckle fracture. For these fractures, the distal fragment tends to shift dorsally; the fractures should be molded in flexion.
- Volar buckle fractures are less common, more difficult for emergency physicians to appreciate, and more likely to be mismanaged; these should be molded in extension.
- Don’t solely rely on the radiologist’s report. It may not offer enough detail. It may be wrong. Make sure you see the X-rays, not just the report!
Introduction
If you see kids in your emergency department, then you’re managing pediatric fractures. Distal radius fractures are the most common.

Fractures can be stable or unstable. Stable fractures will not shift with activities of daily living. They need comfort and protection while healing. A simple dorsal buckle fracture of the distal radius is a good example (as in Case 2).
Unstable fractures have a tendency to shift. Some kids with distal radius fractures need a reduction (not covered in this article). Those cases are more impressive, and it is more intuitive that those fractures have a tendency to shift back to their pre-reduction position and should be molded in the opposite direction to prevent that possible shift.



4 Responses to “Emergency Medicine Pearls, Pitfalls for Treatment of Pediatric Distal Radius Fractures”
November 19, 2017
Matt JaegerThanks so much! I appreciate your article very much. I often treat simple buckle fractures with a removable splint, but after reading your article I wonder if I may have done the same with a volar buckle fractures in the past. I will certainly change my practice. Thanks again.
July 30, 2018
Arun SayalThanks Matt.
There are tons of little pearls from our specialist colleagues – subtleties that help us manage us patients better.
Glad it helped.
Arun
November 19, 2017
AWHGreat article, and has absolutely changed my practice. Thank you Dr. Sayal!
July 30, 2018
Arun SayalThanks AWH!