Barb sheath technique (see Figure 4). Normally, this is reserved for small hooks that are not embedded in the nose, in the ears, or near joints, as this is a more technically difficult technique that may cause further damage from blindly inserting an 18-gauge needle to disengage the barb. Firmly grasp the shaft end with the needle driver. Inject 0.5–1 mL of local anesthetic (without epinephrine) along the entry wound site of the fishhook. Insert an 18-gauge needle along the entry site, with the bevel facing toward the barb. Once the core of the needle has engaged the barb, slowly retract both the hook and the needle back out through the entry site.4
Explore This Issue
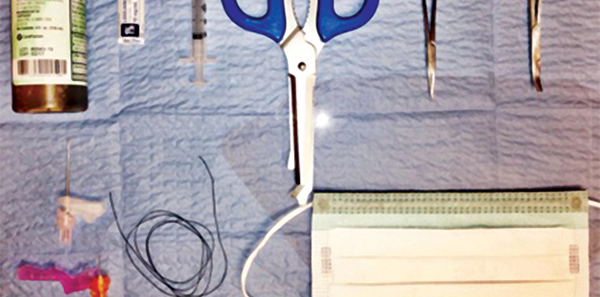
ACEP Now: Vol 35 – No 06 – June 2016String yank technique (see Figure 5). This is likely the least painful technique for removing fishhooks. Although effective, this technique cannot be used on hooks embedded in ears, the nose, or joint cavities and is more suited for single hooks that are embedded into stable surfaces such as arms, the back, and the scalp region.6 Both the patient and the provider should wear eye protection. After cleaning up the area as previously described, loop a string around the bend of the hook. With your nondominant thumb or index finger, depress the shaft of the hook toward the embedded body part until it is parallel to the surface to disengage the hook. With a quick and firm jerk of the string, using your dominant hand, remove the hook. Local anesthetic is applied similarly to other techniques at the provider’s discretion. Many patients do not require an anesthetic, as experienced fishers often perform this procedure in the field.4
Case Conclusion
The fishhook is safely removed using the string yank technique. A dry dressing is applied, and the patient’s tetanus vaccine is updated. The fishhook was embedded superficially, therefore no prophylactic antibiotics are given. The patient will live to boast the big one next time.

Dr. Trinh works at Saint Barnabas Hospital in Livingston, New Jersey.
 Dr. McNamee is an attending physician at Emergency Medicine Professionals in Ormond Beach, Florida.
Dr. McNamee is an attending physician at Emergency Medicine Professionals in Ormond Beach, Florida.
 Dr. McGovern is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
Dr. McGovern is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
References
- Doser C, Cooper WL, Edinger WM, et al. Fishhook injuries: a prospective evaluation. Am J Emerg Med. 1991;9(5):413-415.
- Swanson JL, Augustine JA. Penetrating intracranial trauma from a fishhook. Ann Emerg Med. 1992;21(5)568-571.
- Blaivas M, Lyon M, Brannam L, et al. Water bath evaluation technique for emergency ultrasound of painful superficial structures. Am J Emerg Med. 2004;22(7): 589-593.
- Reichman E. Fishhook removal. Emergency Medicine Procedures. New York, NY: McGraw-Hill Education/Medical; 2013.
- McClary D. Saltwater fishing tips, tackle and techniques. Accessed May 12, 2016.
- Buttaravoli P, Leffler SM. Fishhook Removal. Minor Emergencies. Philadelphia, PA: Elsevier/Saunders; 2012:543-546.
Pages: 1 2 3 4 | Single Page




No Responses to “Emergency Medicine Techniques, Equipment List for Removing Fishhooks Lodged in Patients”