
The evidence is in. We need more women emergency physicians.
Explore This Issue
ACEP Now: Vol 35 – No 04 – April 2016There is a marked gender discrepancy in emergency medicine. Although females comprise 50 percent of medical school classes, they make up only 25 percent of EM-trained physicians (see Table 1). An even smaller percentage of women are in major leadership positions within EM (see Table 2).
While emergency medicine has made some progress in the quest to increase the number of women in the workforce, it has not succeeded at the rate the specialty needs nor has it reached anticipated outcomes based on the pipeline of women medical students.
Without the full participation of women in EM, the nation’s ability to provide emergency care will be stretched even further. EM must attract and retain women physicians while concurrently addressing their unique needs in order for professionals to provide medical care for the millions of patients who annually visit the nation’s emergency departments.
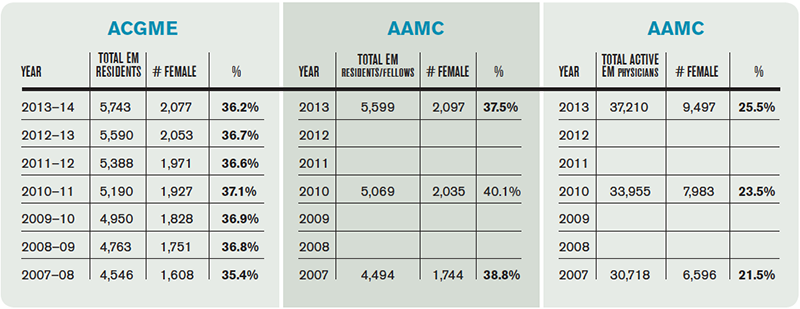
(click for larger image) Table 1. Annual Number of Women in Emergency Medicine
As the nation adapts to meet unprecedented challenges of health care, teams should include women physicians not only because more emergency physicians are needed within the medical community but because the ideas, skills, interests, and creativity women bring are essential to the ongoing success of the specialty.
Be cognizant of the fact that women leaders are the best tool to improve recruitment and retention of women.
Women especially appreciate the need for work-life integration and have already provided guidance for the implementation of processes that support life “balance,” and these concepts represent best practices for both men and women. In fact, millennials of both genders appreciate and agree on the need for work-life integration.
Investing in women physicians for the long term is key. Research shows that women may take off more time early in their careers but that they take off less time later in their careers as compared to men.
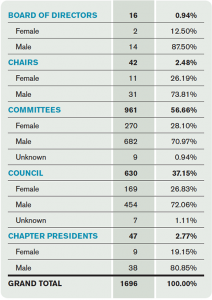
(click for larger image) Table 2. Women in EM Leadership Positions
Improving Recruitment and Retention of Women Emergency Physicians
Fortunately, there is a lot that can be done. The list below is not exhaustive, but it provides a good starting place.
- Include positives about emergency medicine opportunities for work-life balance in recruitment.
- Ensure that maternity/paternity leave policies are in place.
- Include information regarding maternity/paternity leave, accommodations for pregnancy-associated needs, and family leave as a standard part of the recruitment package so applicants don’t have to ask.
- When an emergency physician informs her group of pregnancy, the first response should be “Congratulations!” followed by assurance that maternity/paternity policies are available and that it is expected that they will be used.
- Remove any stigma associated with taking maternity/paternity leave.
- Monitor the use and advertise the utility of family-related policies to ensure that all employees feel comfortable using them without penalty.
- Ensure female involvement in recruitment, and when possible, pair women with female mentors for at least the first year after starting a new position.
- Be cognizant of the fact that women leaders are the best tool to improve recruitment and retention of women.
- Encourage involvement in Women in Medicine groups, such as ACEP’s American Association of Women Emergency Physicians, Society of Academic Emergency Medicine’s Academy for Women in Academic Emergency Medicine, Association of American Medical Colleges’ Group on Women in Medicine and Science, and social networks like FemInEM blog and Physician Moms Group. Also encourage home institutional opportunities.
- Make it a point to highlight any recent progress made for women physicians at your place of work. Recognize and promote the added value women bring to the department.
- Work to improve work-life integration in your department/institution.
- Integrate and allow part-time positions for physicians who need this option.
- Experiment with changes in practices that are out of step with the realities of modern life and work to create environments that foster success for all the physicians in your group. (Yes, the emergency department has to be staffed for the present, but by making incremental adjustments now, you will help ensure the future staffing of the emergency departments of the future.)
- Conduct periodic audits to check for unjustified gender disparities in compensation.
- Implement family-supportive scheduling practices for all physicians. For example:
- Schedule critical departmental meetings and functions during hours typically covered by school/child care services, and allow meetings to be conducted and attended via phone or electronic media.
- Explore and consider implementing child care subsidy programs for all employees (eg, dependent care flexible spending accounts).
- Explore and advertise options for emergency/backup dependent care for employees.
- Develop a policy that supports the needs of employees experiencing a significant life event. Such a program may include offering support surrounding devastating illness or death of loved one; guaranteeing physicians paid time off for family leave around the birth/adoption of a child; treating medical and family leave similarly in terms of paid time off, backup coverage, and flexible scheduling; offering graduated return to work after a significant life event; and offering job shares or flexible scheduling for the first six months after the birth or adoption of a child.
- Modify clinical staffing patterns and personal shift requirements (eg, set schedules) to minimize physical stress on pregnant staff. Consider taking pregnant women off overnight shifts during the third trimester.
- Provide clean, private non-bathroom facilities for lactation within or immediately adjacent to the emergency department. Ensure physicians are able to leave the department during their shift for lactation needs without compromising patient care.
- Create and implement supportive work policies and a stable income when physicians experience a significant life event (ie, family crisis, an increase in work burden at home, or an event such as pregnancy, birth, or adoption).
Bottom line: More women physicians in emergency medicine are needed. The consequences of neglecting to address the unique needs of women in emergency medicine will negatively impact the ability to recruit and retain emergency physicians and will ultimately affect the ability to provide medical care for the millions of patients who need emergency care.
Pages: 1 2 | Single Page



11 Responses to “Emergency Medicine Workforce Needs More Women Physicians”
April 25, 2016
Dan MarcusSo basically, this article could be shortened to read “men should be prepared to pay for women to be off to have a baby and men should work more night shifts to make it easier for their pregnant colleges.” The article suggests that if these changes aren’t made, then patient care will suffer. I don’t support the subsidizing of coworkers life choices. I would,however, work extra if my college is unable to whether they are male or female.
April 30, 2016
MB LynchWow! Who pissed you off? Do you have any children? How would you feel about the mother of your child risking her life and your child’s life because they were so extremely over worked? Have you ever been pregnant? Breast feed a child or been so engorged you wanted to cry?
The author is not saying that men pick up the night shifts, but that everyone (including the non pregnant females) help out for a few weeks for the mother and child’s health. Just like we do for our colleagues with family and personal emergencies.
You don’t want to pay for my life choices? You mean you don’t want to pay for me to create a life? How about if you get cancer (knock on wood) because you smoke…can I refuse you disability.? Additionally, I pay for short term disability so that I could take maternity leave.
Women now make up 60% of medical schools. Therefore, if medicine is going to survive it needs to start to adjust to accommodate women doctors and our “choices to create life.” If men gave birth I am sure they would demand better maternity leave and you would not have to pump in a bathroom. I’m sure you’d have a recliner with epsn on a flat screen.
Get pregnant, give birth and breast feed a child…then get back to me.
Women and their pesky uteruses are here to stay…get used it to it.
May 8, 2016
Mark BuettnerWow! MB Lynch what a fantastic emotional rant that was. It was perfectly devoid of reason. Kudos to you. Let me give you some answers:
1) I would be very upset if the mother of my child was risking her life and my childs life. I would not tolerate it at all as a matter of fact.
2) I would advocate for women not to have children if they live a lifestyle that that places a life threat to them and or their unborn children. This just makes sense doesn’t it?
3) I probably should have to tell you but I will remind you that Men cannot have babies. Nor can we breast feed babies. We don’t have the right plumbing.
4) Yes, I think you should be able to refuse to pay for somebody’s disability. That should be the responsibility of Dr. Marcus. This would be similar to you taking time away from work should be your responsibility. I am willing to bet that he would agree with me.
5) If you are asserting that Medicine is at risk for not surviving because women now make up 60% of Medical Students, perhaps we should seek out more men to enter the field.
Glad to help,
Sincerely,
Mark.
May 8, 2016
Mark BuettnerDitto Dr. Marcus.
May 8, 2016
georgeI respect all the issues.The gender equality issues should not include pregnancy and time off issues. The numbers are correct and there is a gender gap.I on the other hand see a greater crisis.I am a Black male in the field of EM.I have watched the numbers of women leap over the years yet the percentage of African American males in the field is at a critical joke level.Women complain about their poor numbers but you are more likely to see a patient with ebola than a Black ER doc….it is just the truth.I respect the issues of women I am just waiting to turn over a patient to a doctor of color before I retire.
May 9, 2016
EM DocI agree in equality, but to critique objectively, the author doesn’t mention percent of women applying to EM residency. If it’s 50:50, then sure – good article. If it’s 30:70 women to men, then are we already being given preferential treatment (36% women residents)? It would be interesting if anyone has the data…
May 9, 2016
JDAWomen with “their pesky uteruses” can then work jobs where their uteruses don’t get in the way. Equality means equality, not one group subsidizing another. Women may be 60% of medical school graduates but they are not 60% of the work force because they CHOOSE to balance their life based on multiple factors, one of which is having children. Part of physician shortage is due to having 60% women in Medical School and then that 60% is only working part-time. Not a good plan for a national work-force issue. Finding a colleague who is willing to work nights and weekends and long stretches and extra shifts makes that person marketable. If you CHOOSE to have kids, try to be super-mom, expect your colleagues to work around you and your personal life, you have made yourself less marketable. That is not gender inequality, it is marketability. Until women are willing to sacrifice personal goals for professional goals they will not be able to be represented equally. To me that is fair, not sexist.
May 12, 2016
el rubioMy residency director in New York City would roll over in his grave. I remember a female resident once called in sick for PMS and another senior female resident drove to her apartment and physically dragged her back to work. I have not missed a day of work in 25 years.
May 12, 2016
el rubioIn my experience pregnant students residents and physicians are very reluctant to risk exposure to infectious diseases such as TB HIV Trauma Meningitis Chicken Pox Mumps Plague Ect. This forces me to risk my life more often then usual.
August 1, 2016
EM resI would work extra shifts to cover any male coworker who just had a baby and wanted to take time off, the same I would for a female coworker.
Commenters: stop seeing everything as man vs woman and a little more about having some humanity. It might make your life better, too.
February 14, 2018
Craig L. BosleyThis is a sexist statement.
Ethical Statement –
Emergency needs more good emergency physicians.