The Case: A 58-year-old male presents to the emergency department in cardiac arrest after sustaining a stab wound to the left neck (zone 1). The patient was apneic with a faint pulse at the scene but arrested en route to the emergency department. Medics have the patient intubated, and two large-bore IVs have been initiated with crystalloids infusing. He is still pulseless in the emergency department. A focused assessment with sonography for trauma (FAST) exam is negative. After brief resuscitative efforts in the trauma bay, the patient is pronounced dead.
Explore This Issue
ACEP Now: Vol 36 – No 07 – July 2017Forensic Pearls
A stab wound is a form of sharp-force trauma caused by a thrusting action whose injury length on the body surface is less than its depth of penetration into the body. The force is delivered along the long axis of a narrow, sharply pointed object. The impact force is concentrated at the tip of the object—and the sharper the tip, the more easily it can penetrate the skin. Stab wounds can be homicidal, self-inflicted, or accidental. Internal and external hemorrhage are of concern when treating stabbing victims. Knives tend to make up the majority of weapons used in stabbings. However, any pointed object can be a weapon (eg, pencil, screwdriver, barbecue fork, scissors, awl, etc.).
The skin edges of a stab wound are called the wound’s margins, and the ends or tips are the wound’s angles. The length of the wound is measured from one angle to the other. A line drawn between the two angles is the long/longitudinal axis. The longitudinal axis can be described as vertical, horizontal, or angled. The width is the widest measurement between the two margins.
Several factors should be considered when determining the characteristics of a stab wound. These include motion used, force applied, sharpness/dullness of the tip, type/nature of the weapon, and type/nature of tissue encountered.
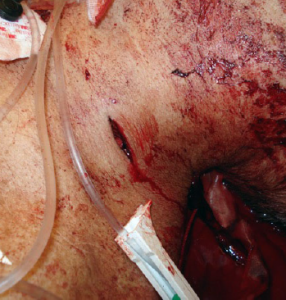
A 58-year-old male with a stab wound to the left neck (zone 1).
PHOTO: Ralph Riviello
There are several things that can be learned about the weapon from looking at the wound itself. However, determining the dimensions of the weapon and depth of penetration are not among them. This is due to the effect of elasticity of skin shrinking slightly on withdrawal of the object (by up to 2 mm). Also, when the blade has entered the skin at an oblique angle, the length of the entry slit may be longer than expected. Skin elasticity and Langer’s lines (orientation of collagen fibers in the dermis) can cause wounds to gape, contributing to miscalculations. If the weapon has not fully entered the skin, the wound depth will correspond to the part that has penetrated the skin and will not represent the maximum length of the weapon. In addition, objects are rarely pushed into the body and withdrawn at exactly the same angle, and rocking of the knife distorts a wound’s appearance. Finally, compressible body parts, like the abdomen or chest wall, often indent during the stabbing, and thus the area penetrated can be at a depth greater than the weapon.
Characteristics of Stab Wounds
- Stab wounds have clean-cut edges.
- Single-edge knives (like kitchen knives) cause wounds that have a clearly pointed edge.
- Serrated knives may leave serrations when the knife has been drawn over the skin surface. This is, however, not a consistent feature of serrated knife stab wounds, and they are usually indistinguishable from wounds caused by other single-edge knives.
- Knives or weapons with two sharp edges (double-edge blades), such as military knives, bayonets, and ceremonial daggers, show pointed edges on both sides of the wound or a spindle-shaped entry slit tapered at both ends.
- Knives with blade guards (at the handle end closest to the blade) can produce distinctive bruising/abrasions to the side of one of the wound angles.
- Bruising may also be present where the assailant’s fist impacts against the skin during the stabbing, depending on the amount of force used and depth of weapon penetration.
- Wounds caused by other implements may cause patterned wounds characteristic of the sharp end of the weapon, such as an X-shaped wound from a Phillips head screwdriver.
- Traditional screwdrivers and chisels usually produce rectangular wounds with abraded margins.
- Ice picks and awls produce wounds that can be mistaken for small caliber gunshot wounds (rounded defect surrounded by thin rimmed abrasion).
- Scissors may produce different wounds depending upon their design and position (open or closed) at the time of the injury. Closed scissor wounds are single and Z-shaped. Open scissor wounds are paired, with varying distances between the pair.
- Barbecue forks will produce paired stab wounds with a fixed distance between the pair. Forks should produce wounds that match the number of tines, maintaining a fixed distance between the wounds.
Forensic Documentation
When caring for a stabbing victim, there are several forensically important considerations. Stab wounds should be documented in terms of their anatomic position and their relative position to fixed anatomical landmarks. The overall wound length, width, and directionality should be documented and the appearance of the wound’s margins and angles described. If the wound is gaping, the margins can be held together to better evaluate the wound angles. This can be done by simply holding the margins together or using clear tape over the wound. If there are multiple stab wounds, each needs to be documented separately. Preprinted body diagrams/drawings can be used for documentation, and of course, photographic documentation should be used whenever possible.
Pages: 1 2 | Single Page



No Responses to “What Emergency Physicians Can Learn from Stab Wounds”