Previously called reflex sympathetic dystrophy (RSD) or causalgia, complex regional pain syndrome (CRPS) entails severe and chronic pain and disability involving a part or whole of a limb. The pain follows a non-dermatomal distribution. CRPS-1 (reflex sympathetic dystrophy) is the most common, accounting for approximately 90 percent of cases, and differs from CRPS-2 (causalgia) in that a nerve lesion typically from trauma, vascular event, or surgery is identified in the latter. Approximately 60 percent of cases involve the upper limbs, with 40 percent affecting a lower limb. CRPS typically follows a minor or moderate extremity injury, such as a wrist fracture, sprain, blunt injury, stabbing, animal bite, or elective surgery. In a minority of cases, no inciting event can be recalled or identified. The disorder typically starts within four to six weeks of the injury. Most patients with CRPS report that pain caused them to stop working.1 It may follow a stroke or myocardial infarction (“shoulder-hand syndrome”). The incidence has been reported to be as high as 28 percent following Colles’ fracture, although most cases resolved after one year. Approximately 3 to 5 percent of patients who sustain a distal radius fracture develop CRPS.2-4 Muscle weakness and changes in sweating and hair and nail growth may occur in that limb.4 Allodynia is defined as pain induced by non-painful stimuli (painful touch), whereas hyperalgesia is more pain than expected to be induced by painful stimuli. One or both should be present in making this diagnosis. Continuing pain in CRPS is disproportionate to the inciting event. Pain, sensory, trophic (hair growth increase, changes in nail growth), and motor symptoms are not confined to single nerve innervation territories.3 Vasomotor findings may include temperature asymmetry, skin color changes, sweating changes/asymmetry, or edema.5
Explore This Issue
ACEP Now: Vol 35 – No 12 – December 2016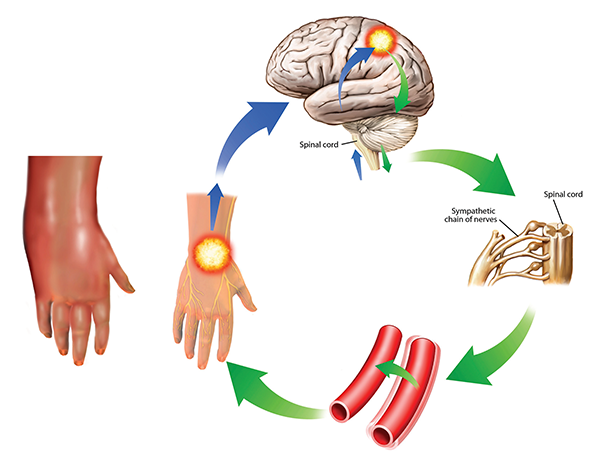
Complex regional pain syndrome
This condition is also known as reflex sympathetic dystrophy. The symptoms can worsen over time and spread through the body as they are reinforced in the cycle shown here. The sympathetic response (green) from the brain (upper right) to the pain impulses (blue) cause vessel spasms (lower right) that increase the pain. In this case, the pain and swelling are in the hand, but other areas of the body can also be affected. It is severely painful and treatment is difficult, involving drugs, electrical stimulation, and psychological and neurological forms of therapy.
John T. Alesi / Science Source
There may be objective findings in the patient with CRPS—for example, side-to-side difference in skin temperature, or osteopenia and osteoporosis with abnormalities on bone scan/scintigraphy or on plain X-rays with both hands on one film. Other potential testing may include MRI, which may demonstrate bone marrow edema and autonomic testing of sweat output. The diagnosis of CRPS is excluded by the existence of another condition that would better explain the degree of pain and dysfunction.6 Women are affected more often than men. It is most frequent in those ages 61 to 70.7 Approximately 20 percent of patients are able to resume previous activities.8
Pages: 1 2 3 4 | Single Page




No Responses to “What Emergency Physicians Need to Know About Complex Regional Pain Syndrome”