
2. Medications used to lower BP are also important. The majority of patients’ BP was lowered with urapidil (61 percent) with a minority being treated with nicardipine (8 percent). How would this data extrapolate to North America, where nicardipine is a commonly used medication, while urapidil is not available in the United States or Canada?
Explore This Issue
ACEP Now: Vol 42 – No 10 – October 20233. Bundle: The bundle treatment included addressing hypertension, hyperglycemia, pyrexia, and hypercoagulability. Which part of the intervention caused the benefit? We have seen other bundles, in conditions like sepsis, that did not ultimately turn out to be better than usual care (ARISE, ProMISe and ProCESS).4 There could also be a Hawthorne Effect because this was unmasked trial and participants and clinicians knew whether they were receiving bundled care or usual care.
4. Outcome Assessment: The primary outcome in this trial was an ordinal analysis of the mRS score. Concerns have been raised about ordinal analyses. Dr. Rory Spiegel, who does the podcast for Annals of Emergency Medicine with Dr. Ryan Radecki, has written about this issue of ordinal analyses.5,6
There are also the issues with the mRS score itself for inter-rater reliability. Scoring of mRS, even by a neurologist, is only moderately reliable at best when done face-to-face.7 Similar issues with the mRS have been reported by others.7
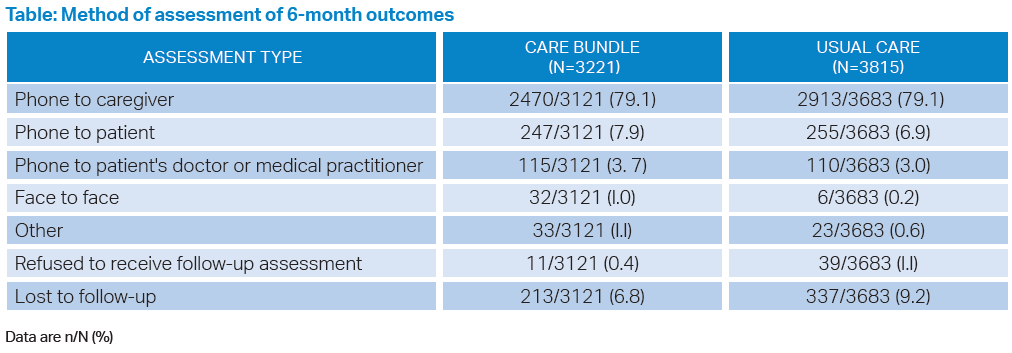
In INTERACT-3 the outcome assessment is done via caregiver over the phone (79 percent of the time) or with the patient over the phone (7 percent of the time) and not face-to-face (less than 1 percent of the time). (See table) This should decrease our confidence in the primary outcome of mRS at six months.
Click to enlarge.
Bottom Line
Intense blood pressure lowering in patients with ICHs continues to seem safe if we do not overshoot our target BP and cause hypotension, but we are still uncertain if it provides a patient-oriented outcome of benefit.
Case Resolution
The patient has severe disease with a poor prognosis. There is no definitive evidence to inform our management. You have a conversation with the neurological critical-care team and discuss what will be a mutually agreeable treatment plan.
Thank you to Dr. Mike Pallaci who is both a professor of emergency medicine for the Northeast Ohio Medical University, and an adjunct clinical professor of emergency medicine for the Ohio University Heritage College of Osteopathic Medicine, for his help with this critical appraisal.
Pages: 1 2 3 4 | Single Page



No Responses to “Goal-Oriented, Bundled Care For Intracerebral Hemorrhage Improves Outcomes”