
A 76-year-old female presents to the emergency department obtunded with left hemiplegia. Symptoms began just prior to presentation. Her blood pressure (BP) is 195/104 mmHg. The CT scan reveals a hemorrhage in the right internal capsule, suggestive of acute hypertensive hemorrhagic stroke. Should the BP be treated aggressively, what is the target, and how quickly should we achieve that target?
Explore This Issue
ACEP Now: Vol 42 – No 10 – October 2023Background
There have been a couple of large and influential trials published on BP management after an intracranial hemorrhage (ICH). Both INTERACT-2 and ATACH-2 showed no statistical difference in their primary outcome between intensively lowering the BP and a less-intensive strategy.1,2
The 2022 AHA/ASA Guidelines give several recommendations on this topic.3 The class (strength) of their recommendation is 2a/2b based upon Level B and Level C quality of evidence. The language used in the guidelines is important. The specific language used in the AHA/ASA guidelines is as follows:
- “In patients with spontaneous ICH in whom acute BP lowering is considered, initiating treatment within 2 hours and reaching target within 1 hour can be beneficial to reduce the risk of HE [hematoma expansion] and improve functional outcome”
- Class 2a recommendation, “Moderate”: is reasonable, can be beneficial; level of evidence C-LD (limited data)
- “In patients with spontaneous ICH of mild to moderate severity presenting with SBP [systolic BP] between 150 and 220 mmHg, acute lowering of SBP to a target of 140 mmHg with the goal of maintaining in the range of 130 to 150 mmHg is safe and may be reasonable for improving functionaloutcomes.”
- Class 2b recommendation, “Weak”: may be reasonable, may be beneficial, effectiveness not well established; level of evidence B-R (randomized; moderate quality evidence from 1 or more randomized controlled trials or meta-analyses of moderate-quality randomized controlled trials)
- “In patients with spontaneous ICH presenting with large or severe ICH or those requiring surgical decompression, the safety and efficacy of intensive BP lowering are not well established.”
- Class 2b recommendation, “Weak”: may be reasonable, may be beneficial, effectiveness not well established; level of evidence C-LD (limited data)
Clinical Question
Can the implementation of a goal-directed care bundle, incorporating protocols for early, intensive BP lowering in addition to management algorithms for hyperglycemia, pyrexia, and abnormal anticoagulation, implemented in a hospital setting, improve outcomes for patients with acute spontaneous intracerebral hemorrhage?
Reference
Ma LM, Hu X, Song L, et. al. The third intensive care bundle with blood pressure reduction in acute cerebral haemorrhage trial (INTERACT3): an international, stepped wedge cluster randomised controlled trial. Lancet. 2023;402(10395):27-40.
- Population: Patients 18 years of age and older, presenting within six hours after the onset of ICH
- Exclusions:
- Definite evidence that the ICH is secondary to either a structural abnormality in the brain or previous thrombolysis
- Attending clinician felt there was a high likelihood that the patient would not adhere to the study treatment and follow-up regimen
- Exclusions:
- Intervention: Bundled care per a goal-directed intensive care protocol to correct hypertension, hyperglycemia, pyrexia, and hypercoagulability, with the goal of achieving treatment targets within one hour of initiating treatment and maintaining them for seven days (or until discharge or death, whichever came first)
- Comparison: Usual care at the discretion of the treating physician
- Outcome:
- Primary Outcome: Functional recovery measured at six months according to the modified Rankin Scale (mRS) score and analyzed as an ordinal outcome (shift across all categories)
- Secondary Outcomes:
- Functional recovery according to a shift analysis of scores on the National Institutes of Health Stroke Scale at seven days
- Dichotomous mRS outcomes at six months (0-2 versus 3-6, and 0-2 versus 3-5)
- Death at six months
- Death or neurological deterioration at seven days
- Health-related quality of life using the EuroQoL Group 5-Dimension self-report questionnaire
- Residence at six months (own home versus other)
- Time to hospital discharge
- Safety Outcomes: All-cause and cause-specific serious adverse events, recorded for the duration of follow-up
- Type of Study: A pragmatic, international (10 countries), multicenter (121 hospitals), unmasked, stepped-wedge, cluster randomized, controlled trial
Authors’ Conclusions
“Implementation of a care bundle protocol for intensive blood pressure lowering and other management algorithms for physiological control within several hours of the onset of symptoms resulted in improved functional outcome for patients with acute intracerebral haemorrhage. Hospitals should incorporate this approach into clinical practice as part of active management for this serious condition.”
Results
A total of 7,036 patients were recruited from 121 hospitals that could be included in the modified intention-to-treat analysis. The mean age of patients was 62 years with 36 percent female. Most of the patients (over 90 percent) were Chinese.
Key Results
The odds of a poor functional outcome were lower in the care bundle group compared to usual care.
- Primary Outcome: mRS favored the care bundle group (OR, 0.86; 95 percent confidence interval, 0.76-0.97; P = 0.015), consistent across all adjustments and calculations.
- Secondary Outcomes: Most secondary outcomes did not show a statistically significant difference. Some showed trends in a positive direction. Patients who received the intervention were statistically more likely to be discharged by day seven. The EuroQoL Group 5-Dimension self-report questionnaire quality of life assessment was a mixed bag, but the effects on this scale diminished when they made the various statistical adjustments in their posthoc analysis.
- Safety Outcomes: There were significantly fewer serious adverse events in the bundled care group.
EBM Commentary
1. External Validity: It is unclear if this data applies to patient you see in your emergency department. One reason is where these patients were recruited to be included in the trial. The cohort came from nine low- and middle-income countries and one high-income country. Most of the patients were recruited from China (90 percent) with only 3 percent coming from Chile (the only one classified as a high-income country).
2. Medications used to lower BP are also important. The majority of patients’ BP was lowered with urapidil (61 percent) with a minority being treated with nicardipine (8 percent). How would this data extrapolate to North America, where nicardipine is a commonly used medication, while urapidil is not available in the United States or Canada?
3. Bundle: The bundle treatment included addressing hypertension, hyperglycemia, pyrexia, and hypercoagulability. Which part of the intervention caused the benefit? We have seen other bundles, in conditions like sepsis, that did not ultimately turn out to be better than usual care (ARISE, ProMISe and ProCESS).4 There could also be a Hawthorne Effect because this was unmasked trial and participants and clinicians knew whether they were receiving bundled care or usual care.
4. Outcome Assessment: The primary outcome in this trial was an ordinal analysis of the mRS score. Concerns have been raised about ordinal analyses. Dr. Rory Spiegel, who does the podcast for Annals of Emergency Medicine with Dr. Ryan Radecki, has written about this issue of ordinal analyses.5,6
There are also the issues with the mRS score itself for inter-rater reliability. Scoring of mRS, even by a neurologist, is only moderately reliable at best when done face-to-face.7 Similar issues with the mRS have been reported by others.7
In INTERACT-3 the outcome assessment is done via caregiver over the phone (79 percent of the time) or with the patient over the phone (7 percent of the time) and not face-to-face (less than 1 percent of the time). (See table) This should decrease our confidence in the primary outcome of mRS at six months.
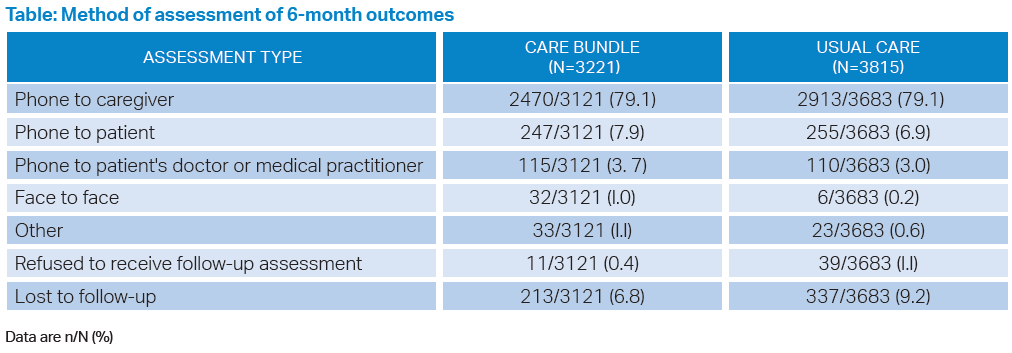
Click to enlarge.
Bottom Line
Intense blood pressure lowering in patients with ICHs continues to seem safe if we do not overshoot our target BP and cause hypotension, but we are still uncertain if it provides a patient-oriented outcome of benefit.
Case Resolution
The patient has severe disease with a poor prognosis. There is no definitive evidence to inform our management. You have a conversation with the neurological critical-care team and discuss what will be a mutually agreeable treatment plan.
Thank you to Dr. Mike Pallaci who is both a professor of emergency medicine for the Northeast Ohio Medical University, and an adjunct clinical professor of emergency medicine for the Ohio University Heritage College of Osteopathic Medicine, for his help with this critical appraisal.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
References
- Anderson CS, Heeley E, Huang Y et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355-65.
- Qureshi AI, Palesch YY, Barsan WG, et al. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N Engl J Med. 2016;375(11):1033-43.
- Greenberg SM, Ziai WC, Cordonnier C, et al. 2022 guideline for the management of patients with spontaneous intracerebral hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2022;53(7):e282-e361.
- ARISE Investigators; ANZICS Clinical Trials Group; Peake SL, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371(16):1496-506.
- Spiegel R. The adventure of the cardboard box. EMCrit website. http://emcrit.org/emnerd/the-adventureof-the-cardboard-box/. Published June 30, 2013. Accessed September 17, 2023.
- Spiegel R. A Secondary Examination of The Adventure of the Cardboard Box. Published November 10, 2014. Accessed September 17, 2023.
- Quinn TJ, Dawson J, Walters MR, et al. Reliability of the modified Rankin Scale: a systematic review. Stroke. 2009;40(10):3393-5.
Pages: 1 2 3 4 | Multi-Page



No Responses to “Goal-Oriented, Bundled Care For Intracerebral Hemorrhage Improves Outcomes”