RAPTIR is a novel block that targets the same distal portion of the brachial plexus while correcting for the major challenges associated with traditional ICB and AXB. The patient is allowed to remain in the position of comfort during the procedure, and the needle angle is kept flat relative to the ultrasound probe, markedly increasing needle tip visualization and avoiding a trajectory deep into the thoracic cavity. Additionally, the needle path avoids the nearby cephalic vein and thoracoacromial artery, and only one injection is required to block the entire distal extremity.
Explore This Issue
ACEP Now: Vol 37 – No 10 – October 2018We have successfully performed the RAPTIR in numerous patients in our emergency department, facilitating dense anesthesia and ideal pain control for closed reductions. When compared to procedural sedation, we have noted two specific benefits from using the RAPTIR. First, when attempting to optimize closed reduction (and potentially avoid subsequent open reduction and internal fixation), we often require repeat radiographs to confirm proper alignment. RAPTIR allows for essentially painless repeat reduction attempts (if needed) without worry of a prolonged sedation. Second, because we use a long-acting anesthetic for the block, patients can be sent home with excellent pain control, starting an oral analgesic before the block wears off.
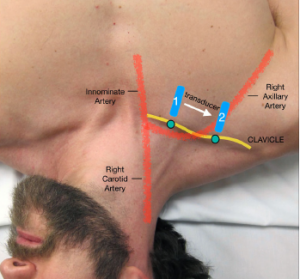
Figure 1: Overview of the initial and final probe position when performing the block. Slide the transducer (blue solid line) from mid-clavicle region to the deltopectoral groove. The probe marker (green dot) should face cephalad. The goal is to visualize the subclavian/axillary artery as it exits below the clavicle.
Credit: Luftig, Mantuani, Nagdev

Figure 2: Stand above the patient with the ultrasound screen in clear view. Note the transducer is located in the deltopectoral groove with the needle entering above the clavicle.
Credit: Luftig, Mantuani, Nagdev
Procedure
Visit www.highlandultrasound.com/raptir for a video demonstration of this technique.
Pre-assessment: Patients with a short, poorly mobile neck; thick chest wall; or deformed clavicle, such as from prior fracture, are poor candidates for RAPTIR, and another technique should be considered. We recommend a pre-block survey scan to determine if the axillary artery is clearly visible (see Figure 1).
Positioning: Place the patient in a semi-recumbent supine position with the affected extremity adducted in a position of comfort. Rotate the patient’s head away from the injured limb and put a folded blanket under the upper back (ipsilateral to the injury). Stand at the head of the bed with the ultrasound system in direct line of sight (on the same side as the injured extremity) (see Figure 2).
Pages: 1 2 3 4 5 | Single Page




2 Responses to “How to Effectively Block an Acutely Fractured Distal Radius”
November 4, 2018
Mark BaileyNice if the ED MD can have a specialist come down. Too much time wasted for a real ED.
November 4, 2018
Michael Anthony MaciasLove this block and looking forward to incorporating into my practice though probably should reserve for more complex injuries as majority of distal radius fractures are easily reduced comfortably with a simple hematoma block.