Ultrasound-guided nerve block (UGNB) is an extremely useful technique for emergency physicians as a multimodal approach to the acutely injured patient. In the emergency department, UGNBs are an adjunct for pain management and can be an ideal way for clinicians to reduce the overreliance on systemic opioids.1–3 In patients with contraindications to procedural sedation, UGNBs may also be the only suitable method for targeted analgesia. Recent end-point data indicate early ultrasound-guided femoral nerve blocks improve functional outcomes in patients with hip fractures, making the integration into emergency medicine practice imperative.4 Unfortunately, despite evidence indicating both the feasibility and utility of UGNBs in the ED management of the acutely injured patient, reports indicate poor penetration in emergency medicine clinical practice.5
Explore This Issue
ACEP Now: Vol 37 – No 07 – July 2018In our 10-year experience with UGNBs, we believe that one of the major limitations for physicians is the lack of a simple location for all supplies needed to perform a UGNB. Using basic design thinking methodology to streamline the process for the clinician, we developed prearranged block bags that contain the basic supplies needed to perform a UGNB.
Our block bags contain the minimum supplies necessary for a basic ED-based UGNB. All anesthetics remain in our ED automated medication dispensing system until ordered by the clinician. Weight-based dosing parameters and a preprocedural timeout checklist are not placed in the block bag but are easily located online to simplify the process. Lipid emulsion (20%) is kept with our anesthetics, and all providers who are performing UGNBs are familiar with dosing if there is concern for local anesthetic systemic toxicity (see www.lipidrescue.org for details). A standard ED policy should be in place with dosing guidelines and references whenever anesthetics are used (ultrasound-guided or landmark-based).
Assembling the Bag
- Each block bag contains (see Figure 1):
- Two 20-cc syringes
- 20-g 3.5-inch blunt-tip block needles
- IV extension tubing
- Two 10-cc normal saline (NS) flushes
- 18-g needle
- Tuberculin (TB) or insulin needle/syringe (for skin wheal)
- Transparent dressing for probe
- Alcohol pads and clorhexadine swab
- Body marking pen

Figure 1: The various labeled components are placed in a specimen bag so that clinicians can quickly grab supplies for a UGNB. Anesthetic is ordered by the clinician and brought to the bedside by the nurse.
Procedural Tips
- Consent should always be obtained before performing a UGNB.
- A discussion with consulting services (orthopedics, general surgery, etc.) and determination of which injuries are (and are not) ideal for UGNBs should be performed in advance of performing the procedure.
- Scan the patient to determine the location of the nerve. Position the patient and ultrasound screen to allow for optimal ergonomics. We recommend that the ultrasound screen and site of injection be in direct view of the clinician so that minimal head movement is needed to perform the block. In most cases, this would mean that the ultrasound system is contralateral to the site of injury.
- The patient should be placed on a cardiac monitor for the duration of the block and for about 10 to 15 minutes after completion.
- Once the ideal location and needle pathway has been determined, a skin wheal should be placed at the expected site of needle entry.
- For a low-volume block (10 cc or less), a single operator technique can be used (needle on syringe), as shown in Figure 2.
- For a higher-volume block (10–20 cc anesthetic), we prefer a two-operator technique (hand on needle), as shown in Figure 3.
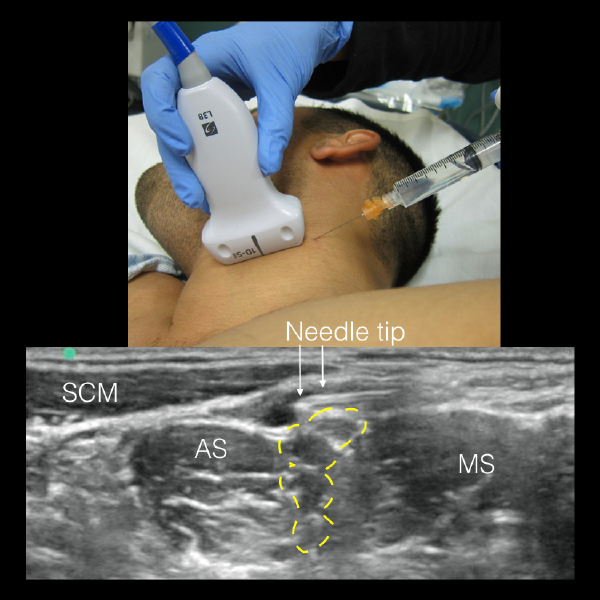
Figure 2. For low-volume blocks (less than 10 cc), we recommend a single-operator technique. A two-operator technique (see Figure 3) can be used if the operator is a novice and would benefit from normal saline (NS) hydrodissection to ensure proper needle visualization. The operator is using an in-plane technique to perform an interscalene brachial plexus block. SCM: sternocleidomastoid muscle; AS: anterior scalene muscle; MS: middle scalene muscle; yellow dashed line: brachial plexus at the level of the interscalene muscles.
Pages: 1 2 | Single Page




No Responses to “How to Implement Ultrasound-Guided Nerve Blocks in Your ED”