
Clinical Presentation
The patient may present with small amounts of blood from the trachea/ET tube (sentinel bleed), or with frank hemoptysis. There may be pulsatile movements of a tracheal cannula.
Explore This Issue
ACEP Now: Vol 43 – No 03 – March 2024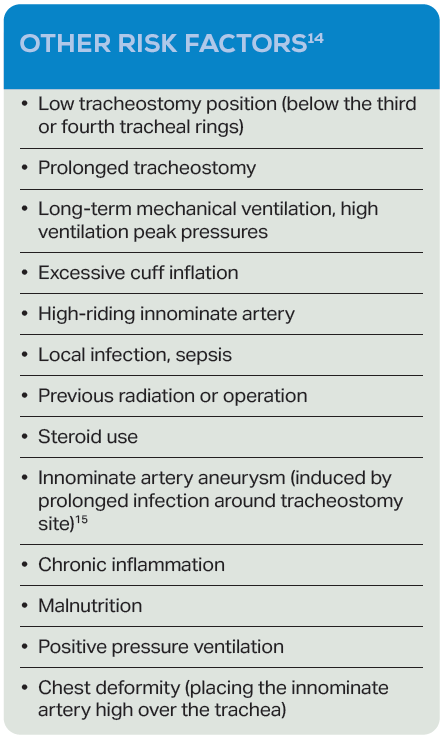 TIF classically develops from three days to six weeks after tracheostomy or insertion of a cuffed endotracheal tube. The clinical manifestation may be either sudden massive tracheal hemorrhage at the tracheostomy site and/or from the endotracheal tube, or a warning/sentinel bleed. Approximately 35-50 percent of patients develop a sentinel bleed prior to life-threatening hemorrhage.11
TIF classically develops from three days to six weeks after tracheostomy or insertion of a cuffed endotracheal tube. The clinical manifestation may be either sudden massive tracheal hemorrhage at the tracheostomy site and/or from the endotracheal tube, or a warning/sentinel bleed. Approximately 35-50 percent of patients develop a sentinel bleed prior to life-threatening hemorrhage.11
Risk Factors for Development of TIF
High cuff pressures have been implicated, and it is recommended that pressure in a tracheostomy cuff be maintained at less than 20 mm Hg.12 Attention to cuff pressure and tracheal injury appears to stem from the 1970s.13
Emergency Management
The immediate management includes overinflation of the cuff of the tracheostomy or endotracheal tube, and aspiration of blood to clear the airway. The inflation of the tube is done blindly, without any set volume, until the bleeding is stopped. In patients with a tracheostomy in place, use of a tracheostomy cannula with a wired silastic tube has been described to adjust the position of the cuff and using cuff over-inflation to provide hemostasis.4
Maximal inflation of the ETT balloon should be below the level of the tracheostomy. The cuffed tube may be inserted deep into the opening and the cuff expanded, followed by trying the maneuver moving the tube up and re-inflating if the bleeding is not controlled initially. An option if overinflating the tracheostomy cuff does not stop the bleeding is to insert a cuffed oral tracheal tube translaryngeally, then advancing it so that the balloon lies distal to the tracheostomy stoma but above the carina, and withdrawing the tracheostomy tube in order to facilitate simultaneous translaryngeal tracheal intubation. The balloon cuff should be expanded excessively from the lower portion of the bleeding area to prevent accumulation of blood in the lungs.10
If bleeding continues, pressure should be applied to the stoma site. These measures have been reported to control bleeding 80 percent of the time.16 If the patient is hemodynamically stable to undergo bronchoscopy, the major threat to the patient becomes respiratory compromise, so it is recommended to leave the tracheostomy tube in place.5
Manual compression of the innominate artery at the level of the tracheal stoma/manubrium is the Utley maneuver, which applies only for patients who have a tracheal/tracheostomy stoma. Digital compression consists of inserting a finger into the pretracheal space to tamponade the innominate artery against the posterior manubrium or sternum.17 Compression of the innominate artery against the posterior sternum may require enlarging the tracheostoma.18 The finger is inserted through the stoma alongside the endotracheal tube and, while 90 percent success rate has been reported with this method in controlling bleeding, the pressure must be maintained until the patient is transferred to the operating room.10 If a tracheostomy site is present, local compression with a Foley catheter balloon through the tracheostomy site has been described.15
Pages: 1 2 3 4 5 | Single Page



No Responses to “How To Manage Tracheo-Innominate Fistula”