
Injuries or soft tissue infections of the lower extremity are common reasons for patients to seek emergency care. Ultrasound-guided regional anesthesia is a key component of multimodal and opioid-sparing pain control in the emergency department.1 Femoral, fascia iliaca, and posterior tibial blocks are lower extremity blocks performed routinely in many emergency departments.2
Explore This Issue
ACEP Now: Vol 39 – No 08 – August 2020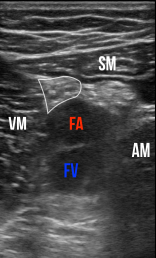
Figure 2: Transverse sonographic view of the adductor canal. The sartorius muscle (SM) forms the “roof.” Vastus medialis (VM) is medial, and the adductor magnus (AM) is lateral. The saphenous nerve (white outline) lies between the femoral artery (FA) and the sartorius. FV is the femoral vein.
images: Peter Croft and David Mackenzie
Blocking the saphenous nerve, often called an adductor canal block, is another valuable tool for emergency clinicians. At the level of the adductor canal, the saphenous nerve is a terminal sensory branch of the femoral nerve. A block provides anesthesia to the medial aspect of the lower leg and ankle as well as the skin overlying a portion of the patella. It is effective for laceration repair or abscess drainage in this distribution and can be used for adjunctive pain relief postoperatively in knee surgeries.3 The adductor canal block is commonly used for analgesia in patients undergoing partial or total knee replacement surgery. Unlike a femoral nerve block, strength in the quadriceps is unaffected, allowing early mobilization or discharge. As with other nerve blocks, ultrasound guidance allows operators to visualize the nerve and can increase the efficacy and safety of the block.1,4
Equipment
Transducer: Select a high-frequency linear transducer (15-6 or 10-5 MHz) with the nerve or soft tissue preset.
Anesthetic: Options include a short- or long-acting anesthetic. Choice depends on the goal of the nerve block: pain relief (preferentially a longer-acting anesthetic) or procedural (preferentially a shorter-acting anesthetic).
- Long-Acting:
- Ropivacaine (max. dose 3 mg/kg), anticipate 6–10 hours analgesia
- Bupivacaine (max. dose 2 mg/kg), anticipate 3–12 hours analgesia
- Short-Acting:
- Lidocaine (max. dose 3 mg/kg), anticipate 1–3 hours analgesia
Research supports using low-dose perineural dexamethasone to prolong the duration of peripheral nerve blocks for several hours.5 A safe choice would be the addition of 2–4 mg of dexamethasone to the volume of anesthetic.
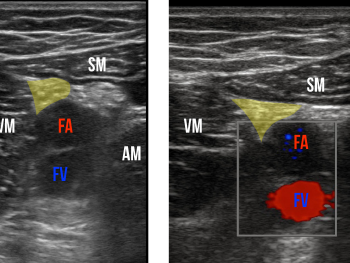
Figure 3: Sonographic view of the adductor canal. The saphenous nerve is highlighted.
Figure 4: Color Doppler flow visualized in the femoral artery and vein. The target saphenous nerve is marked in yellow.
Needle: Choose a 21-gauge or larger needle to optimize visualization. In patients with more soft tissue, a spinal needle may be needed. Consider bringing up a skin wheal of lidocaine to make needle entry less painful. When available, nerve block needles increase echogenicity and may help with visualization, though they are not required to perform an adequate block.
Pages: 1 2 3 | Single Page




No Responses to “How to Perform an Adductor Canal Nerve Block”