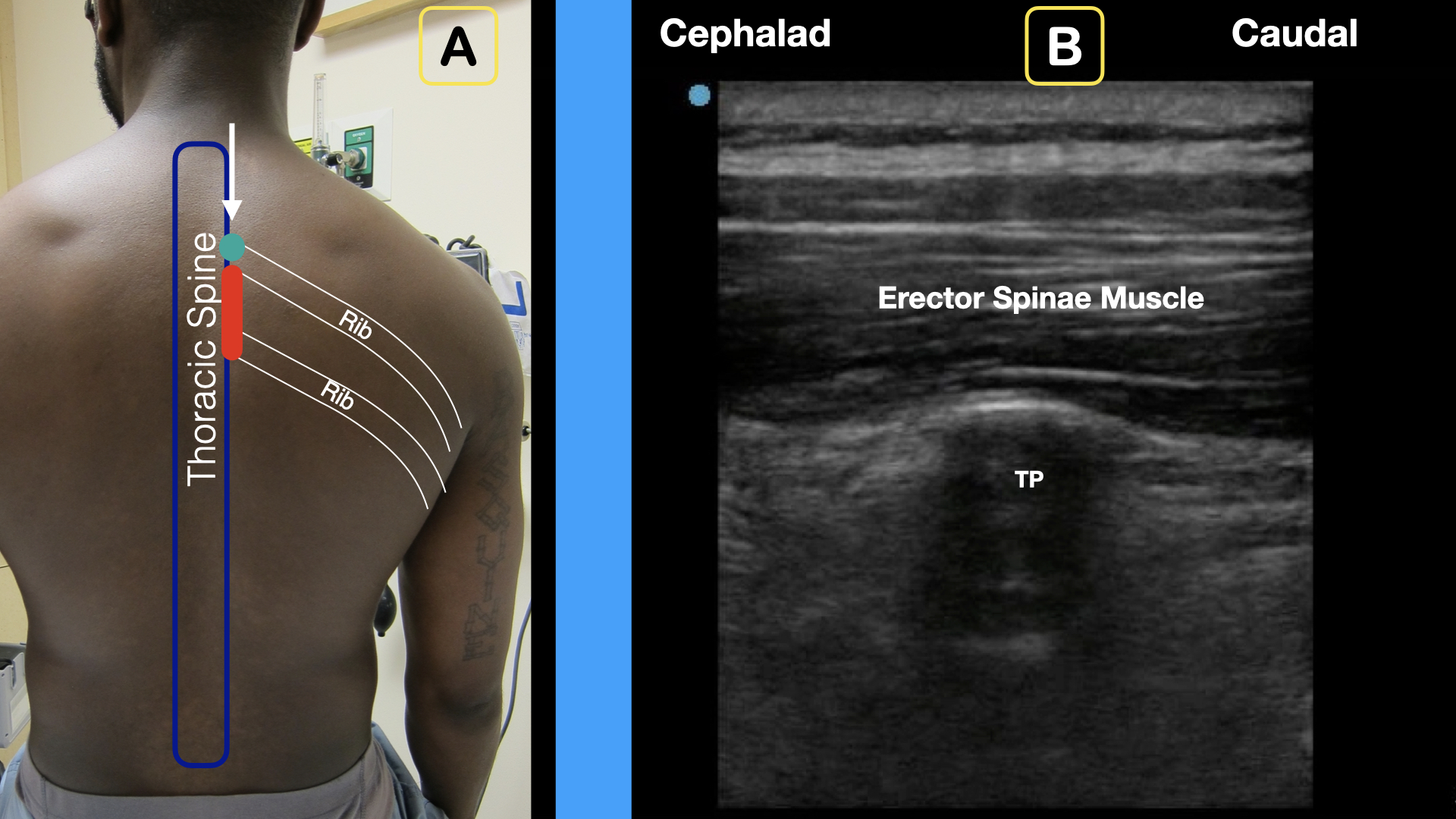
Start with the probe in longitudinal orientation over the ribs, midway between the scapula and the spine. Note that deep to the ribs, the pleura can be easily identified. Carefully slide the probe medially, looking for the deeper costotransverse junction and then the transverse process (more superficial, wider, and rectangular). If the transducer is placed too medial (past the transverse process), the more deeply located lamina will come into view. The clinician should also note the erector spinae muscle that sits directly over the transverse process. Scan again, back and forth, to differentiate between the deeper (laterally located) rounded ribs with underlying pleura and the targeted, more superficial, and rectangular transverse process, a view in which the pleura is often not visualized (see Figures 4 and 5).
Explore This Issue
ACEP Now: Vol 40 – No 09 – September 2021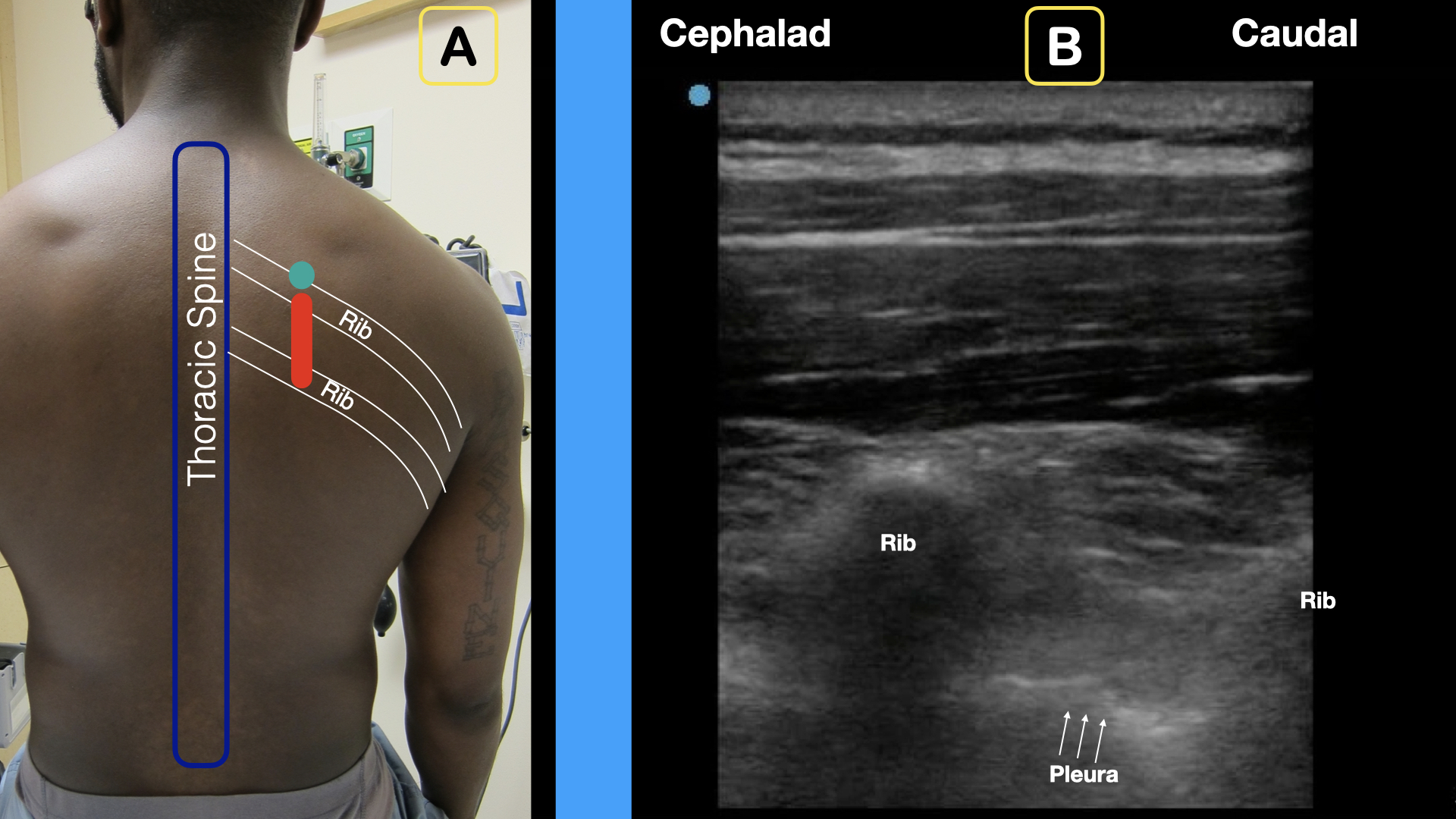
(click to enlarge)
4A) The longitudinal transducer (with probe marker facing cephalad) is placed between the spine and scapula.
4B) Note the ribs (with shadow) and pleura.
Credit: Arun Nagdev
(click to enlarge)
5A) Slide the probe medial until the transverse process is clearly visualized.
5B) The rectangular transverse process (TP) is noted. The erector spinae muscle will sit just superficial to the TP.
Credit: Arun Nagdev
- Skin Wheal
After satisfactory identification of the transverse process (and the overlying erector spinae muscle), widely prep the skin with chlorhexidine, allow it to dry completely, and place a 2–3-mL lidocaine skin wheal 2–3 cm cephalad to the transducer.
- Needle Entry
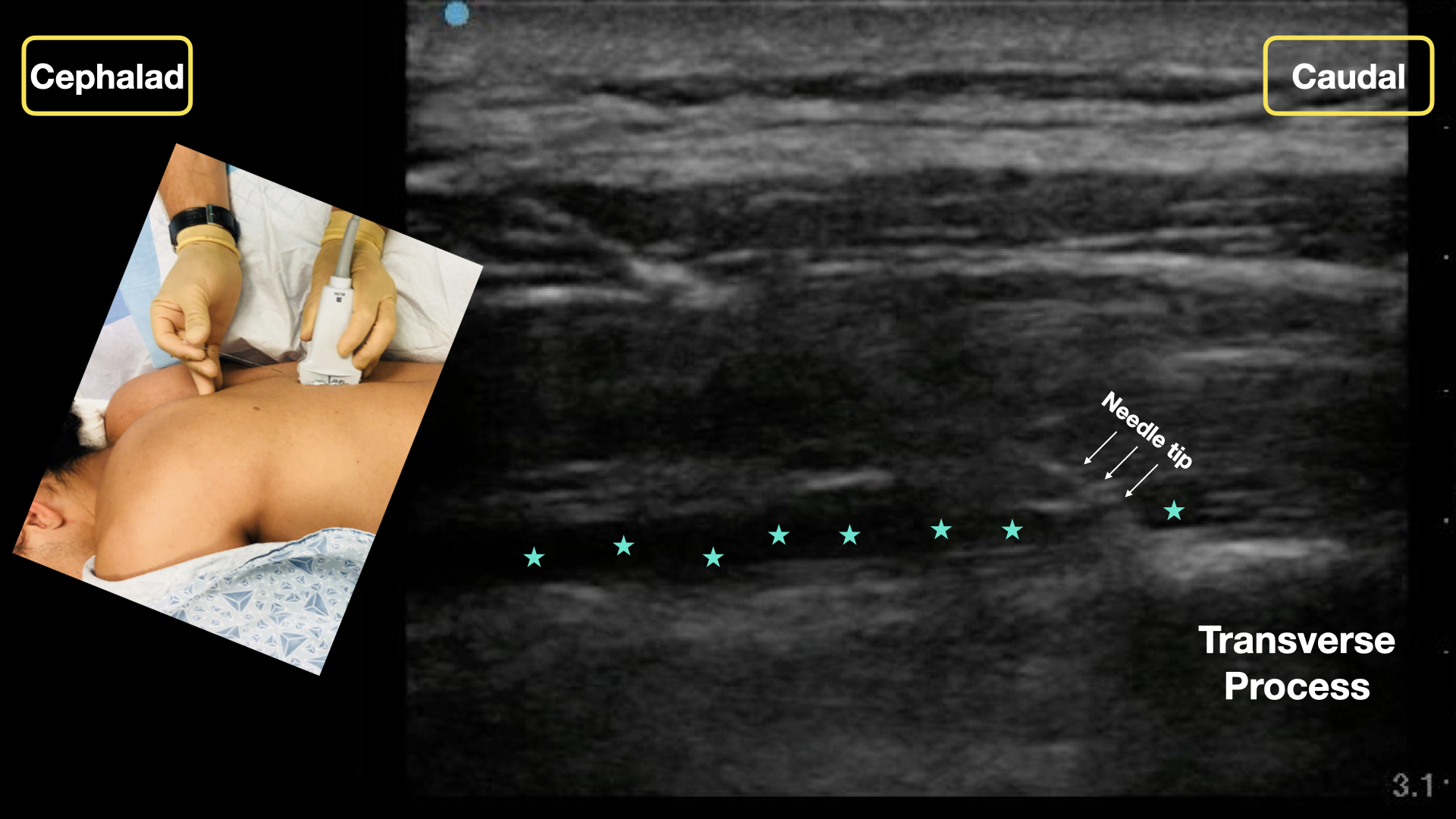
Using an in-plane approach, advance the block needle at a 30º to 45º angle through the trapezius and rhomboid (for blocks at T7 or higher) and then through the erector spinae muscle until the needle tip reaches the posterior surface of the transverse process. After aspiration to ensure no vascular puncture, small aliquots of normal saline are injected to hydrodissect the fascial plane that separates the erector spinae muscle and the transverse process. In our experience, targeting the needle tip at the edge or corner of the rectangular transverse process allows the injectate to hydrodissect the fascial plane more easily. Ensure that the injected anechoic fluid is not placed in the erector spinae muscle but rather is deposited along the fascial plane (see Figure 6, opening of the fascial plane with needle in view). Once satisfied with needle placement, slowly inject the remainder of the 20–40 mL of local anesthetic into the already-open fascial plane.
(click to enlarge)
An in-plane cephalad to caudal approach with clear needle tip is recommended. Note the needle tip and anechoic anesthetic tracks in the fascial plane (green stars).
Credit: Arun Nagdev
Summary
The erector spinae plane block is a simple, safe block that can be applied to a wide variety of painful thoracoabdominal conditions. It is unique in its ability to target both visceral and parietal pain and can be a valuable tool for multimodal pain control in the acute setting. Like with other fascial plane blocks, the clinician should be comfortable using high volumes of injectate, hydrodissecting fascial planes, and recognizing that analgesic onset can be delayed.
Pages: 1 2 3 4 | Single Page


No Responses to “How to Perform an Erector Spinae Plane Block”