
FIGURE 2B: The goal is to visualize the needle tip until it touches the clavicle (red line). (Click to enlarge.)[/caption]
Explore This Issue
ACEP Now: Vol 43 – No 02 – February 2024Once the relevant anatomy is located, place a small skin wheal (2 to 3 ccs of anesthetic) at the inferior aspect of the transducer. Along with marking the entry point for the block, this will provide analgesic for the block.
3. Supplies and Anesthetic
The CPB block uses similar equipment as other ultrasound guided nerve blocks:
- An ultrasound system with a high-frequency 15-6 MHz or 10-5 MHz linear transducer on musculoskeletal or soft-tissue setting
- A blunt-tipped needle: preferably a 20- or 21-gauge regional-block needle
- Appropriately sized syringe to draw local anesthetic; we recommend 20 mL
- 10 mL sterile saline flushes for hydrodissection
- Transparent adhesive ultrasound probe cover (Tegaderm or similar)
- Antiseptic (e.g., alcohol, povidone-iodine, chlorhexidine)
- Sterile ultrasound gel. If available, we recommend using ropivacaine (a concentration of 0.25 percent or less) as it has a longer half-life and a better safety profile than bupivacaine. Weight-based dosing should always be used to prevent local anesthetic systemic toxicity.
4. Performing Procedure

FIGURE 3: The ultrasound system screen needs to be in clear line of sight so that the clinician can see both needle and ultrasound
image. (Click to enlarge.)
Before performing the block, make sure the patient has consented, has intravenous access and is placed on a cardiac monitor.
The patient should be in a supine position. The ultrasound system should be placed so that the operator is able to visualize the point of needle entry, as well as the ultrasound screen in the same line of sight. We commonly place the ultrasound system contralateral to the clavicle that will be blocked (based on what is comfortable for the physician) (Figure 3).
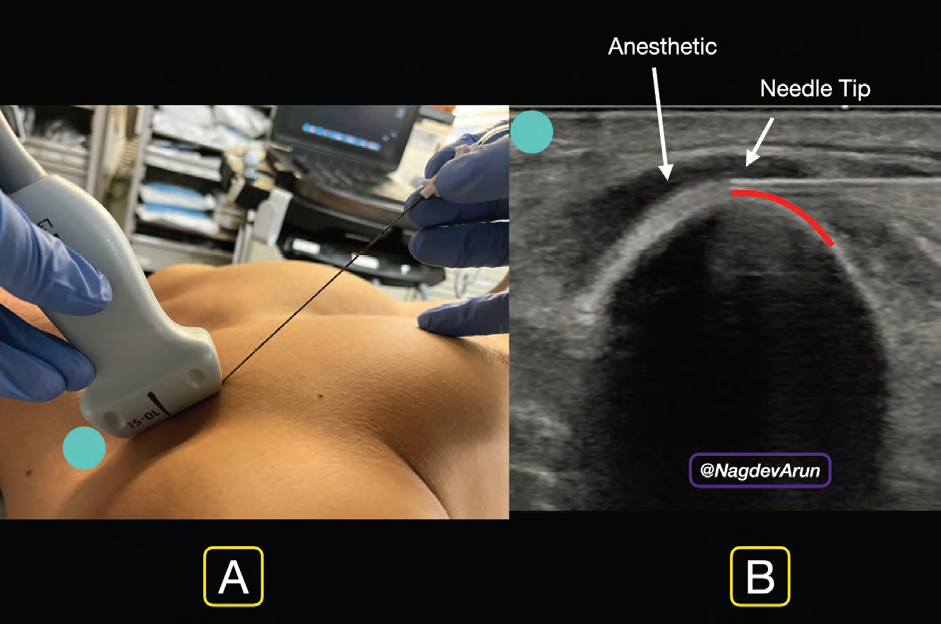
FIGURE 4A: In-plane needle entry.
FIGURE 4B: Needle tip visualized clearly with anesthetic deposited under the clavipectoral fascia. (Click to enlarge.)
Using an in-plane needle approach, enter the skin wheal with a block needle. Visualize the needle tip advancing through the pectoralis major to the inferior aspect of the clavicle (Figure 4A). Ensure continuous needle visualization until the block needle meets the clavicle; resistance may be felt as it goes through the clavipectoral fascia and touches the ostium of the clavicle. We recommend placing the needle at the 12 to 2 o’clock position of the clavicle (Figure 4B). Gently inject 1 to 2 cc of anesthetic to hydrodissect the clavipectoral fascia from the clavicle. The goal is to use the anechoic anesthetic to lift the pectoralis muscle away from the clavicle. This can be visualized with real-time ultrasound guidance. Once the clinician opens this potential space, gently place 3- to 5-cc aliquots, aspirating in between to ensure lack of inadvertent vascular puncture.
Pages: 1 2 3 4 | Single Page



One Response to “How To Perform an Ultrasound-Guided Clavipectoral Block”
February 28, 2024
Doc_CWhy not simply a superficial cervical plexus block more on the caudal side to get the rami claviculares of the cervical plexus?
Cheers