The warm, swollen knee is a common complaint in the emergency department, with joint aspiration being the diagnostic test of choice when a septic arthritis is suspected. Point-of-care ultrasound can accurately determine the presence of a joint effusion as well as guide synovial fluid aspiration.1 The suprapatellar bursa, the largest communicating bursa of the knee joint, allows for a location that is easily visualized with ultrasound and can be rapidly and safely accessed for joint arthrocentesis. A simplified sonographic method for evaluation and aspiration of the knee joint is an important addition for even the most experienced emergency physician.
Explore This Issue
ACEP Now: Vol 34 – No 08 – August 2015Background
The provider must first confirm the presence of an effusion before performing a diagnostic arthrocentesis. Classically, the physical exam findings for a knee effusion are swelling, a decreased range of motion, and a ballotable, or floating, patella. Mimics such as cellulitis, prepatellar bursitis, or abscess that may be difficult to distinguish from joint effusion on physical examination are easily identified with bedside ultrasound.2 Once the presence of a knee effusion has been confirmed, the standard practice for needle arthrocentesis has been a landmark-based approach. Ultrasound has been shown to be effective in identification of knee effusion as well as allow for real-time visualized technique for joint aspiration.3 In the emergency department setting, ultrasound-guided knee arthrocentesis has been shown to help minimize attempts as well as improve procedural confidence in the hands of novice providers.4 Additionally, the suprapatellar approach under ultrasound guidance avoids any tendons or bony or ligamentous structures and facilitates simple and accurate arthrocentesis for the provider.
Mimics such as cellulitis, prepatellar bursitis, or abscess that may be difficult to distinguish from joint effusion on physical examination ar easily identified with bedside ultrasound.
Procedure
Ultrasound Identification of Knee Effusion
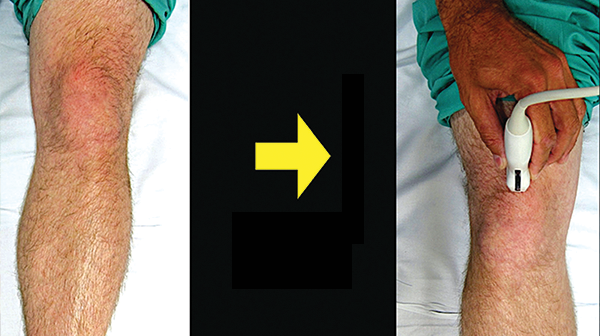
We recommend using the linear transducer (10–5 MHz) for both the identification of the effusion and needle guidance for the arthrocentesis. The patient should be placed in the supine position, with the affected knee slightly flexed (we recommend a small pillow or roll of sheets be placed under the affected knee). Place the linear transducer in the prepatellar fossa in a longitudinal direction with the probe marker caudal (see Figure 1). Identify the patella sonograhically, then slowly slide the probe cephalad until the patella, femur, quadriceps femoris tendon, and fat pad are visualized (see Figure 2). The effusion will appear as an anechoic fluid collection below the fat pad. A small skin wheal of local anesthetic (1–2% lidocaine) injected through a tuberculin syringe should be placed just lateral to the ultrasound transducer (the projected entry point for joint arthrocentesis). We recommend an ultrasound examination of the nonaffected suprapatellar space for comparison.
Pages: 1 2 3 | Single Page




One Response to “How to Perform Ultrasound-Guided Knee Arthrocentesis”
September 30, 2018
CassandraIs ultrasound injection good for ten knee after a keyhole surgery? I had this surgery for sometimes ago and now my left is severe with pain and decided to go for the ultrasound injection.. I had this injection on my shoulder and is good. I had it twice and never back again.So thinking of having one on my knee. Can you
Advise please thanks.