Airway technology has advanced rapidly in recent years and many emergency departments (EDs) now stock video laryngoscopes with hot-swappable disposable blades, second-generation laryngeal masks that are easier to place and designed to transmit an endotracheal tube, and single-use flexible endoscopes that bring the capabilities of conventional fiber-optic bronchoscopes to emergency settings. These advances introduce novel airway management options that are not yet widely utilized.1 One particularly powerful example is the use of a flexible endoscope to facilitate tube delivery after the larynx has been exposed using a video laryngoscope. We call this video-assisted flexible endoscopic intubation VAFEI, pronounced “vaffy.”
Explore This Issue
ACEP Now: Vol 41 – No 11 – November 2022The VAFEI Procedure
Preparation
- Preoxygenate and hemodynamically optimize the patient as time and physiology allow.
- If fully awake approach is undertaken, patient should be pretreated with antisialagogue and diligent topicalization of local anesthesia.
- Equipment list:
- Intubating flexible endoscope (FE) preloaded with endotracheal tube
- Video laryngoscope (VL) blade (hyperangulated geometry particularly advantageous but standard-geometry blade also effective)
- Topical anesthetics (e.g., four percent lidocaine via atomizer) if non-paralyzed approach
- Usual intubation and difficult airway equipment (e.g., suction, capnography, supraglottic device, cricothyrotomy materials)
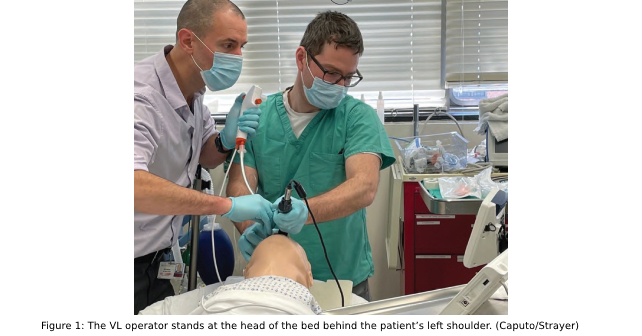
- Positioning (Figure 1):
- VL operator stands at the head of the bed behind the patient’s left shoulder.
- FE operator stands at the head of the bed behind the patient’s head.
- Patient should be positioned in semifowler position.
- Screens (single split-screen is ideal) positioned over the patient’s bed in front of operators.
Airway Pharmacology
- If rapid sequence intubation (RSI) is undertaken, simultaneously administer sedative and paralytic agent.
- If non-paralyzed ketamine-only approach is undertaken, administer dissociative dose or titrated sub-dissociative doses of ketamine until patient is adequately induced.
- Application of atomized lidocaine to the larynx blunts cough and gag reflexes and reduces the chance of vocal cord spasm during ketamine-only approaches.
- When induced, VL operator performs laryngoscopy as usual to obtain adequate view (or, if difficult anatomy prevents adequate view, obtain best possible view). The VL operator, maintaining laryngoscope position with left hand, readies suction in right hand, in preparation for flexible endoscopy.
- Once VL operator obtains their view, the FE operator looks into the mouth, places the scope in the patient’s mouth, and advances to the end of the blade under direct visualization. The FE operator looks at the VL screen to guide the FE to the vocal cords.
- If performing an awake/breathing intubation, vocal cords may be anesthetized with four percent lidocaine via the utility port on the bronchoscope or using a mucosal atomization device.
- The FE operator then advances the FE through the cords, either under guidance of the VL screen or, if VL screen view is inadequate, using the FE screen (see Video 1 and Video 2 on our website).
- The FE operator advances the scope beyond the vocal cords until the carina is visualized.
- The FE operator or assistant railroads the preloaded endotracheal tube (ETT) beyond the vocal cords until the tip is seen on the FE screen.
- The FE operator withdraws the scope, visualizing the tip of the ETT just proximal to the carina to confirm proper positioning.
- The ETT is then attached to a bag valve mask (BVM) or ventilator circuit with waveform capnography to confirm gas exchange.
Pearls and Pitfalls
VAFEI is a simple procedure that can become complex if rushed. The right speed is slower than one’s instincts. Use suction liberally. If the airway is soiled, the VL operator must assertively suction fluids.
Pages: 1 2 3 4 5 | Single Page



No Responses to “How To Use Video-Assisted Flexible Endoscopic Intubation”