Preload the endotracheal tube with the tube’s natural curvature in the conventional orientation, with the bevel facing to the left.
Explore This Issue
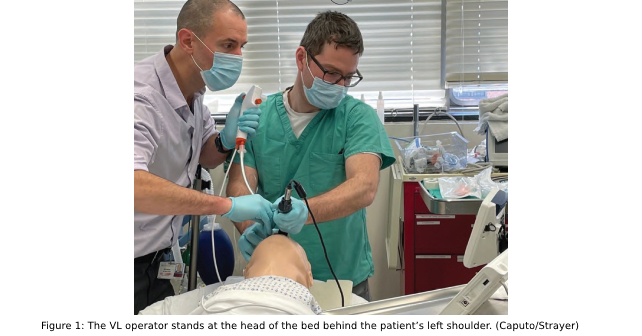
ACEP Now: Vol 41 – No 11 – November 2022Contemporary VL and FE scopes are heated to reduce the likelihood of fogging, but fogging may still occur and is improved by the use of defogging ointment, if available. Alternatively, if fogging of the endoscope occurs, gently press the tip of the scope against the patient’s mucosa to defog. If obstructive anatomy impedes advancing the flexible endoscope, the ETT itself can be used as a conduit; i.e., advance the tube beyond the FE until passage is clear to cords, then advance the scope through the tube and then through the cords. When advancing the tube, if there is a hold-up at the arytenoids, withdraw the tube slightly, then rotate the tube counterclockwise as you advance (left at the larynx, right at the rings for hold-up).2 The VL must be held in place for the entire FE procedure, including as the ETT is railroaded over the scope. Maintaining VL position distracts obstructive tissues and allows visual confirmation of procedural steps.
A convenience sample of 10 patients intubated using the VAFEI technique is described in Table 1.

Click to enlarge Table 1.
Discussion
VAFEI has been described in operating room-based literature, including a randomized controlled trial that demonstrated benefit versus usual video laryngoscopy across a series of outcomes.3,4,5 An emergency department-based case report described the technique with a channeled video laryngoscope, but it has received little attention as an intubation strategy in emergency medicine.6 VAFEI takes advantage of the strengths of each modality to address the weaknesses of the other. Though any blade shape can be used, VAFEI is particularly well-suited for use with hyper-angulated VL (HAVL), as steeply curved blades provide an optimal view of the glottis, but intubation failures and delays with HAVL are often attributable to difficulty maneuvering a styletted ETT to the glottis and then through the cords, down the trachea.7-10 The flexible endoscope overcomes tube delivery difficulties commonly encountered during HAVL as the operator “drives” the scope around the primary and secondary airway curves that confound immobile stylets.11
The use of a video laryngoscope facilitates flexible endoscopy and addresses key barriers to the use of FE in emergency settings. Most importantly, the laryngoscope clears a path through the mouth for the endoscope, allowing it to be manually inserted to the glottic inlet. This obviates the need to navigate the nose and nasopharynx, and reduces the difficulty in steering around the tongue and other oral structures. From an operator skills perspective, VAFEI can be likened to a bougie technique rather than a conventional flexible endoscopic intubation technique.
Pages: 1 2 3 4 5 | Single Page




No Responses to “How To Use Video-Assisted Flexible Endoscopic Intubation”