Explore This Issue
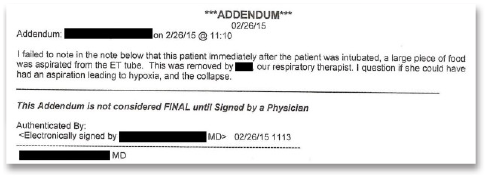
ACEP Now: Vol 40 – No 10 – October 2021Figure 3: Chart addendum about a piece of food in the endotracheal tube during intubation.
The patient survived but suffered a devastating anoxic brain injury and now requires 24-7 care in a nursing home.
The patient’s family filed a lawsuit. They alleged that the physician who cared for her was negligent in giving her hydromorphone, likely contributing to a respiratory arrest. They also allege that the dose of insulin caused a hypoglycemic event that caused cerebral damage. The family also made an accusation of an EMTALA violation for not appropriately screening and stabilizing the patient’s emergency medical condition.
The two sides reached a confidential settlement before trial.
Discussion
This case is unique in that there is no single clear cause of her collapse in the waiting room. There are several credible theories:
- It was later discovered that the patient had an allergy to hydromorphone. However, there was no record of the type of reaction. The way it was previously documented in the medical record meant it did not pull into the emergency physician’s note. While it was technically available for review, this fact was buried deep in the patient’s chart. This highlights the danger of medical software with poor functionality and user interfaces.
- The two doses of hydromorphone could have simply caused respiratory depression. They were given one to two hours before she collapsed in the waiting room. In an otherwise healthy patient, this dose would not be expected to cause apnea, but this patient already had underlying pulmonary edema and complained of shortness of breath.
- She may have aspirated or choked on food in the waiting room. The doctor who ran the code noted that a piece of food was removed from the endotracheal tube. Unfortunately, the physician went back and made an addendum to the chart to mention the possibility of aspiration. This led the plaintiff to suggest that he simply wrote this to try to pass liability to the patient.
- The patient may have suffered an arrhythmia in the waiting room. She had underlying cardiac issues (tetralogy of Fallot), history of cardiac surgeries, and predisposition to hyperkalemia. However, her ECG was reassuring, and she had a normal potassium level before and after the code.
The exact cause of the bad outcome is impossible to determine with any certainty. In all likelihood, it was probably multifactorial. Any one of these factors alone would likely not have caused her cardiac arrest, but the combination of several issues superimposed on her chronically ill state were ultimately catastrophic. Emergency physicians are wise to document carefully and understand the implications when making delayed addenda in the medical record. While correcting medical records when something has been left out is certainly appropriate, these will be viewed very suspiciously in retrospect.
Read the full medical record from this case.
Pages: 1 2 3 | Single Page



One Response to “Lesson Learned: Delayed Documentation Can Lead to Suspicion”
October 24, 2021
Anthony PohlgeersThere will always be suspicion in anything we document. Not documenting this finding would also be suspicious; especially if it came out in RN or RT testimony later. This addendum was timed appropriately and certainly while the patient was fresh to the ICU and when ‘final outcome’ could not have been known by this physician. My vote would be document this ‘remembrance’ even if suspicion is generated in retrospect.