Explore This Issue
ACEP Now: Vol 36 – No 05 – May 2017(click for larger image)
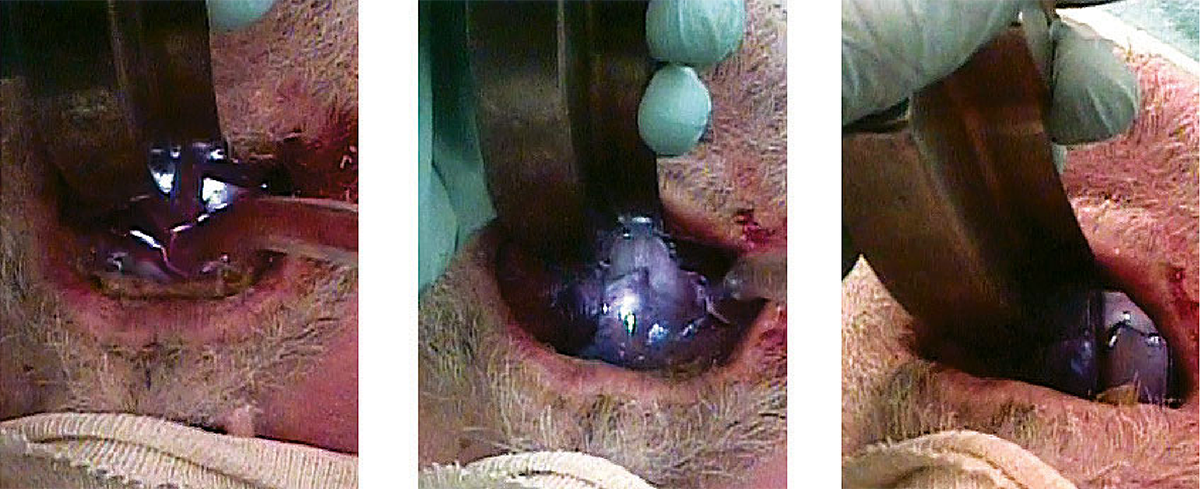
Figure 4: Image sequence for landmark visualization in the setting of massive fluids.
PHOTOS: Richard Levitan
Two final points: Have surgical airway tools ready. If intubation from above is impossible, the only way to oxygenate your patient may be a cricothyrotomy. It should be at the bedside and should be discussed with everyone on the team. This lowers the cognitive threshold for making the decision. Most surgical airways fail not because of technical difficulty but because they are initiated on dead patients. If intubation from above is unsuccessful, cut before the patient codes.
Lastly, gown up and use eye protection. In the words of Mike Tyson, “Everyone has a plan, until they get hit in the face!”
Dr. Levitan is an adjunct professor of emergency medicine at Dartmouth College’s Geisel School of Medicine in Hanover, New Hampshire.
Dr. Chow is assistant professor in emergency medicine/family practice at the Northern Ontario School of Medicine in Thunder Bay.
Dr. DuCanto is a staff anesthesiologist and director of simulation center at Aurora St. Luke’s Medical Center in Milwaukee.
Reference
- Weingart S. A novel set-up to allow suctioning during direct endotracheal and fiberoptic intubation. EMCrit website. Accessed on April 25, 2017.
Pages: 1 2 3 | Single Page




One Response to “How to Manage Fluids in Emergency Airway Procedures”
May 18, 2017
Kyle StricklandAre the authors advocating Preoxygenation of a spontaneously breathing patient with a BVM? I have read that this is superior to NRB but hear many arguments against the use of BVM in spontaneously breathing patients. thanks