The Case
A 49-year-old man presents to the emergency department with an acute onset of back pain. He was carrying some heavy groceries and felt something pull in his lower back. He took some naproxen, which he uses as needed for an old high school football injury, but is still in pain. You do not find any red flags on the history and physical examination. He is feeling better after a dose of morphine, but he still has difficulty bending and walking. It’s time to consider what medications to discharge him home with.
Explore This Issue
ACEP Now: Vol 36 – No 05 – May 2017Background
There are about 2.7 million visits to the emergency department annually for low back pain. While the vast majority of visits are due to benign conditions, this diagnosis can be frustrating for patients and physicians.
One thing physicians have to consider is not missing the uncommon but dangerous conditions like spinal epidural abscess, osteomyelitis, cauda equina syndrome, and pathological fractures. Multiple red flag lists have been published to help physicians identify patients at risk for some of these serious conditions (eg, TUNA FISH, see Table 1). While no list is complete, they can be helpful.
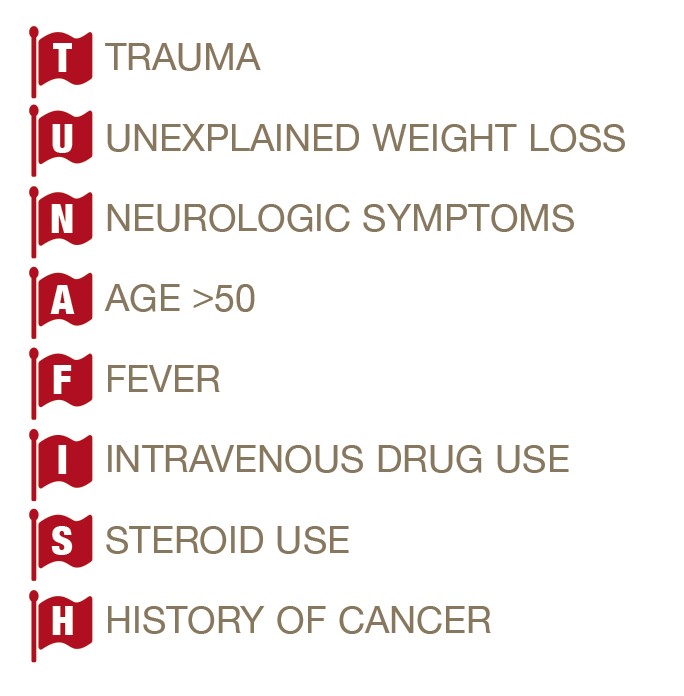
(click for larger image) Table 1: Red Flag Symptoms of Back Pain
Patient demands for imaging can be another source of frustration. The ACEP Choosing Wisely recommendation encourages physicians to avoid lumbar spine imaging:
Avoid lumbar spine imaging in the emergency department for adults with non-traumatic back pain unless the patient has severe or progressive neurologic deficits or is suspected of having a serious underlying condition (such as vertebral infection, cauda equina syndrome, or cancer with bony metastasis).
An additional frustration is the lack of efficacious treatments for low back pain. Acetaminophen has been shown not to affect recovery time compared to placebo.1 Adding cyclobenzaprine or oxycodone/acetaminophen to naproxen alone was shown not to improve functional outcomes.2
There are also concerns about the appropriate use of opioids. ACEP has a clinical policy on prescribing opioids and specifically addresses ED patients with acute low back pain.3 It gives three Level C recommendations:
For the patient being discharged from the emergency department with acute low back pain, the emergency physician should ascertain whether nonopioid analgesics and nonpharmacologic therapies will be adequate for initial pain management.
Given a lack of demonstrated evidence of superior efficacy of either opioid or nonopioid analgesics and the individual and community risks associated with opioid use, misuse, and abuse, opioids should be reserved for more severe pain or pain refractory to other analgesics rather than routinely prescribed.
If opioids are indicated, the prescription should be for the lowest practical dose for a limited duration (eg, one week), and the prescriber should consider the patient’s risk for opioid misuse, abuse, or diversion.
Finally, it is important to be supportive of patients with acute low back pain while at the same time setting realistic expectations. They need to know that their pain may not be 100 percent relieved in the emergency department and that symptoms could persist for weeks or even months.4–6
Clinical Question
In patients with acute nontruamatic, nonradicular low back pain, will a short course of diazepam added to naproxen improve functional outcomes at one week?
Reference
Friedman BW, Irizarry E, Solorzano C, et al. Diazepam is no better than placebo when added to naproxen for acute low back pain (published online ahead of print Jan. 19, 2017). Ann Emerg Med. pii:S0196-0644(16)31214-8.
- Population: Adult patients presenting to the emergency department with acute low back pain ≤2 weeks of duration that caused functional impairment (score >5 on the Roland-Morris Disability Questionnaire [RMDQ]) and discharged home.
- Exclusions: Radicular pain, pain >2 weeks or a baseline low pain frequency of at least once per month, absence of other non-musculoskeletal causes of pain, no direct trauma to the back, unavailable for follow-up, pregnant or breastfeeding, those with chronic pain syndrome, and those allergic or intolerant to the use of the investigational medications.
- Intervention: Educational session, naproxen 500 mg PO every 12 hours as needed, plus diazepam 5–10 mg PO every 12 hours as needed.
- Comparison: Educational session, naproxen 500 mg PO every 12 hours as needed, plus 1–2 placebo every 12 hours as needed.
- Outcome:
-
- Primary: Improvement in the RMDQ score between ED discharge and one week follow-up.
- Secondary: Pain intensity at one week and three months measured on a four-point descriptive scale and adverse events
.
-
Authors’ Conclusions
“Among ED patients with acute, nontraumatic, nonradicular low back pain, naproxen plus diazepam did not improve functional outcomes or pain compared with naproxen plus placebo one week and three months after ED discharge.”
Key Results
The study enrolled 114 patients (mean age mid-30s and about 55 percent men).
Primary Outcome: No improvement in functional outcome at one week when diazepam was added to naproxen. Both groups improved by 11 points on the RMDQ.
Secondary Outcome: Pain intensity at one week and three months was comparable between the two groups. Adverse events were infrequent and comparable between the two groups, with no serious unexpected adverse events reported.
Evidence-Based Medicine Commentary
Inclusion/Exclusion: Only 21 percent (114 of 545) of the patients screened were included in the study. This limits the results to only a specific subset of patients presenting to the emergency department with back pain.
Recall Bias: Many of the inclusion/exclusion criteria and RMDQ were susceptible to recall bias, an error that can occur when participants are asked to remember events or experiences for a study.
Patient Population: Patients were recruited from an urban health care system in a socioeconomically depressed population. Socioeconomic factors may be associated with back pain outcomes, and these results may not necessarily apply to other patient populations.
Unbalanced Groups: Patients in the diazepam arm were more likely to be unemployed. This is a known prognostic factor in recovery in back pain patients.
Blinding: Patients in the benzodiazepine group may have been unblinded. While the authors reported no difference in those feeling dizzy or tired “a lot,” they did not report how many participants felt these side effects “a little.” However, you would expect any lack of blinding to have favored the diazepam group.
Bottom Line
Diazepam should not be routinely added to a NSAID for outpatient management of acute, nontraumatic low back pain patients presenting to the emergency department.
Case Resolution
The man is encouraged to use his naproxen if he feels it provides some benefit, stay active, follow up with his primary care physician, and return to the emergency department if any red flags develop. He also is reassured that symptoms may persist for weeks to months.
Thank you to Anand Swaminathan, MD, MPD, from Core EM and EM:RAP for his help with this review. Dr. Swaminathan is an assistant professor of emergency medicine in the department of emergency medicine at NYU/Bellevue Hospital in New York City.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
References
- Williams CM, Maher CG, Latimer J, et al. Efficacy of paracetamol for acute low-back pain: a double-blind, randomised controlled trial. Lancet. 2014;384(9954):1586-1596.
- Friedman BW, Dym AA, Davitt M, et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA. 2015;314(15):1572-1580.
- Cantrill SV, Brown MD, Carlisle RJ, et al. Clinical policy: critical issues in the prescribing of opioids for adult patients in the emergency department. Ann Emerg Med. 2012;60(4):499–525.
- Itz CJ, Geurts JW, van Kleef M, et al. Clinical course of non-specific low back pain: a systematic review of prospective cohort studies set in primary care. Eur J Pain. 2013;17(1):5-15.
- Donelson R, McIntosh G, Hall H. Is it time to rethink the typical course of low back pain? PM R. 2012;4(6):394-401;quiz 400.
- da C Menezes Costa LC, Maher CG, Hancock MJ, et al. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184(11):E613–E624.
Pages: 1 2 3 4 | Multi-Page



One Response to “Naproxen, Diazepam Evaluated for Treating Acute, Nontraumatic Low Back Pain”
June 30, 2017
jeff wuBefore we remove another medication from our already anemic quiver in the treatment of back pain, I think we have to be more realistic of the goals of the community ED doc. The conclusion of the authors may be correct based on the parameters of the study, but I disagree with their primary end point, and its application to the actual practice of what we do everyday in the ED.
The study focuses on a change in functional outcome at 1 week and 3 months. I don’t know a single practitioner who believes that any treatment we render for back pain in the ED is improving their long-term outcome. Let’s be honest, we just want them to feel a little better right now. What I would like to see is a study to evaluate the change in pain shortly after taking diazepam. If all we cared about was functional outcome at 1 week and 3 months, we should stop prescribing pain medication for fractures, kidney stones, and other painful conditions–at least until a study shows improvement of long-term functional outcome by treating the associated pain with those ailments.
By the way, Anand notes in his blog that the study had a low inclusion rate and did not control for unemployment rate. Perhaps a better powered study that controlled for those types of variables, and gave us a more meaningful end-point would convince guys like me to change my practice.