
A gravid woman presents to your emergency department (ED). Before you can obtain any history, she gives birth in your waiting room. The neonate is apneic and has a heart rate of 48. How do you stabilize this patient?
Explore This Issue
ACEP Now: Vol 43 – No 11 – November 2024Neonatal resuscitation is common; 10 percent of the four million newborns in the U.S. each year will require at least some intervention.1 However, one percent of births will require advanced interventions, including chest compressions, intubation, and medications.2 These rare scenarios are difficult to prepare for; resuscitation guidelines are not strictly followed in more than 90 percent of cases.2 Physicians may experience skill atrophy in these scenarios within two months, underscoring the need for regular review of current guidelines.2
Initial Resuscitation
All necessary personnel and equipment needed for advanced pediatric resuscitation should be present before delivery.4 Immediately after birth, the neonate should be assessed for appearance, pulse, grimace, activity, and respiration (APGAR).5 Cord clamping may be delayed for at least 30 seconds in preterm and term neonates.3 If the neonate is term and has normal tone and breathing and/or crying, they should be placed skin to skin with the mother. Most newborns do not require resuscitative efforts.3
Within 30 seconds, if the newborn has any evidence of apnea, cyanosis, or difficulty breathing, they should be taken to the warmer to maintain a temperature between 36.5–37.5 degrees Celsius and undergo tactile stimulation through drying and rubbing of the back and soles.3,4 Secretions may be cleared and the airway repositioned.3
Advanced Resuscitation
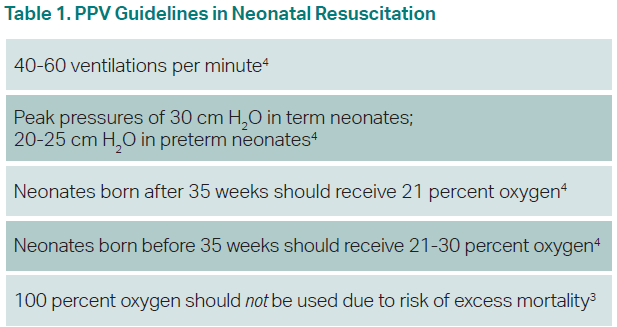
Within 30 seconds of the initial intervention and 60 seconds from birth, the neonate should be reassessed. If the neonate has a heart rate (HR) below 100 or is apneic and gasping, positive pressure ventilation (PPV) should be provided immediately.3 PPV is the most critical step in neonatal resuscitation.2 For every 30 seconds that PPV is delayed, the risk of prolonged admission or death increases by 16 percent.4 A rise in HR is the most important indicator of effective resuscitation. Term infants should initially receive an FiO2 of 0.21 while preterm infants should be started between 0.21 and 0.3, with oxygen titrated based on pulse oximetry. Routine airway suctioning is not recommended. However, if a neonate is delivered through meconium-stained fluid and is showing signs of obstruction during PPV, intubation and tracheal suction can be beneficial.3
Click to enlarge.
PPV is often done incorrectly (Table 1). Two-thirds of cases of continued respiratory depression after resuscitation begins are due to ineffective PPV.2
Pages: 1 2 3 | Single Page



No Responses to “Neonatal Resuscitation Tips”