
Key Result
In adults with OHCAs, survival was more likely with continuous, on-scene resuscitation compared to intra-arrest transport.
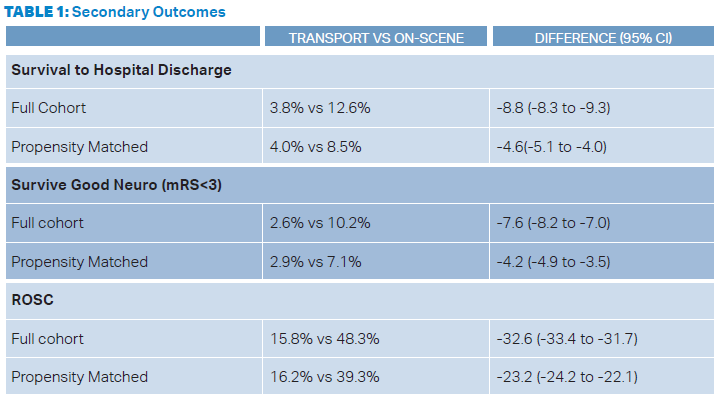
- Primary Outcome: Survival to hospital discharge 12.6 percent on-scene vs 3.8 percent with transport.
- Difference -8.8 percent (95 percent CI -8.3 percent to -9.3 percent).
- Secondary Outcomes: See Table 1.
- EBM Commentary:
- Association is Not Causation: This was an observational study design, which means we cannot conclude causation, but rather only associations. Propensity score matching was done to mitigate some of the biases from non-randomized trials. While these statistical methods can help balance observed baseline covariates, they cannot get to the same level as a randomized control trial.2
- Prognosis Bias: Bias in research can be defined as something that could systematically move the results away from the best point estimate of an observed effect size. Prognosis bias has seven major domains: study participation, attrition, selection of candidate predictors, outcome definition, confounding factors, analysis, and interpretation of results.3 The authors felt that their study could suffer from attrition bias. Adult patients with OHCA and unfavorable phenotypes may have had resuscitation terminated. This means they would not have the opportunity to achieve ROSC. There was a large difference in the termination of resuscitation (0.2 percent of intra-arrest transport compared to 56.7 percent for the on-scene resuscitation).
- Safety of First Responders: While patient care is the primary concern, we must also be concerned about the wellbeing of the EMS paramedics. Providing CPR in the back of a moving ambulance raises concerns about safety. There are data published in Annals of Emergency Medicine reporting an increased odds ratio of crashing with the use of lights and sirens.4 This could lead to increased risk to paramedics who are providing resuscitation during transportation.
SGEM Bottom Line
Low-quality evidence suggests “remain and gain” is associated with better survival to hospital discharge in adults patients with OHCAs compared to “load and go.”
Case Resolution
The paramedic crew stay on scene providing high-quality CPR, identify a shockable rhythm, defibrillate the pitcher, achieve ROSC, and transport the patient to the hospital.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.

Dr. Milne (@TheSGEM) is chief of emergency medicine and chief of staff at South Huron Hospital, Ontario, Canada. He is on the Best Evidence in Emergency Medicine faculty and is creator of the knowledge translation project the Skeptics’ Guide to Emergency Medicine (www.TheSGEM.com).
Pages: 1 2 3 | Single Page




No Responses to “Out-Of-Hospital Cardiac Arrest: Remain and Gain, or Load and Go?”