The Case
A 35-year-old man presents to the emergency department after falling off his bicycle. After basic trauma evaluation, a mildly displaced fracture is noted on the distal third of the clavicle. The patient has moderate to severe pain in that area after intravenous opioid and oral NSAID therapy. A multimodal approach to pain control with an ultrasound-guided superior cervical plexus (SCP) block is offered to the patient.
Explore This Issue
ACEP Now: Vol 33 – No 11 – November 2014Unlike other common nerve blocks, the SCP block does not target an individual nerve but instead targets the fascial plane containing the SCP.
Introduction
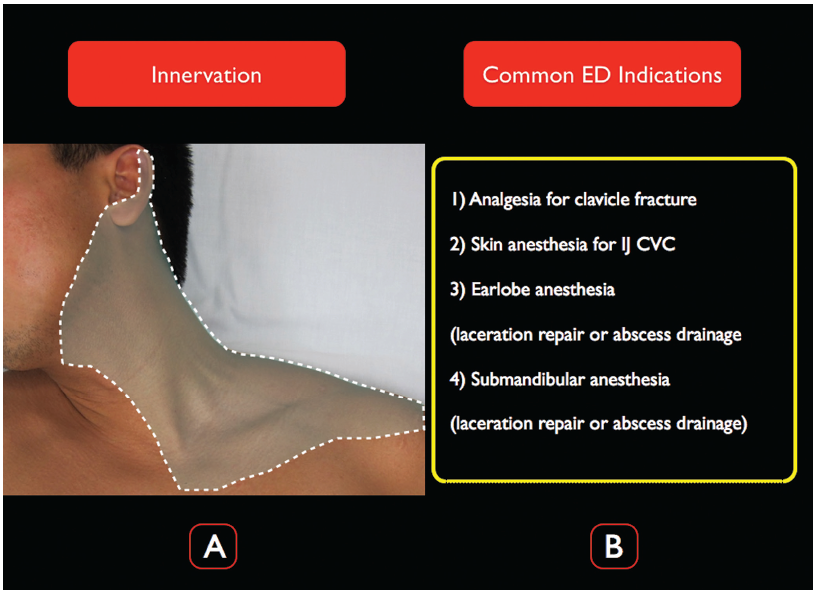
The ultrasound-guided SCP block provides anesthesia to the superficial structures of the neck and shoulder, much of the earlobe, and the superior portion of the shoulder (Figure 1A). In the ED, the SCP block is used for clavicle fracture analgesia, as an alternative to local anesthetic infiltration for internal jugular central venous cannulation (CVC), or abscess drainage/laceration repair on the neck or earlobe (Figure 1B). For clinicians already familiar with performing ultrasound-guided internal jugular CVCs, sonographic localization of the target plane for an SCP block is easily accomplished with a stepwise approach to anterior neck anatomy. Once the emergency physician is comfortable with ultrasonographic needle tip visualization, the SCP block can be rapidly integrated into the clinical armamentarium.
(click for larger image)
Figure 1.
A) The distribution of the SCP block. Note that the innervation extends down to the T2 level and to the cape of the shoulder. B) Common emergency medicine indications for the SCP block.
Anatomy
The superior cervical plexus originates from the C1–C4 anterior rami and emerges from the posterior border of the sternocleidomastoid (SCM) muscle at the level of the superior pole of the thyroid cartilage. The SCP is composed of four distinct nerves: greater auricular (C2, C3), lesser occipital (C2), transverse cervical (C2, C3), and suprascapular (C3, C4). Together, these nerves provide sensory innervation to a large anatomic area including the skin and superficial structures of the neck, the submandibular area, the area overlying the clavicle and upper chest, and portions of the ear and the superior “cape” of the shoulder (Figure 1). Unlike other common nerve blocks, the SCP block does not target an individual nerve but instead targets the fascial plane containing the SCP. Thus, the components of the plexus are not visualized as individual nerves, but instead appear as a poorly defined grouping of hyperechoic structures not readily distinguishable from the surrounding connective tissue. The goal of the block is to place anesthetic in the fascial plane just underneath the belly of the SCM at the C4 level where the SCP emerges along its posterolateral border.
The Procedure
Sterile Preparation. The skin should be prepared with antiseptic solution, and a high-frequency linear (15-6 MHz) ultrasound probe should be disinfected with quaternary ammonia cleaning wipes prior to the procedure. The probe-transducing surface should be covered with a sterile adhesive dressing; a full probe cover is not necessary (Figure 2).
Pages: 1 2 3 | Single Page




One Response to “Pain Control Using Ultrasound-Guided Superficial Cervical Plexus Block”
October 19, 2021
Hazel McArdleCan ultrasound be used for scalene tight muscles