While forearm nerve blocks provide excellent anesthesia for hand injuries (fractures, dislocations, lacerations, abscesses), they don’t provide anesthesia to the volar forearm or the wrist.
Explore This Issue
ACEP Now: Vol 35 – No 10 – October 2016
Hand injuries are a very common emergency department complaint, accounting for a great deal of acute pain as well as chronic morbidity and productivity loss.1–3 Adequate analgesia and anesthesia are necessary to provide hemostasis, wound irrigation, debridement, an adequate examination, laceration or tendon repair, joint reduction, splinting, and other acute interventions. Ultrasound-guided forearm nerve blocks can provide definitive analgesia and facilitate these interventions in acute hand injuries in the emergency department.4–7

Figure 1. Distribution of the median (purpe), radial (yellow), and ulnar (red) nerves on the hand (A) and forearm (b).
Anatomy of Forearm Nerves
The distribution of nerves throughout the forearm is in three segments (see Figure 1):
- Median nerve: radial/lateral aspect of volar hand; volar surface of thumb, index, long, and radial/lateral side of ring finger
- Radial nerve: radial/lateral aspect of dorsal hand; dorsal surface of thumb; dorsal surface of index, long, and radial/lateral side of ring finger, proximal to the distal interphalangeal (DIP) joints
- Ulnar nerve: ulnar/medial aspect of dorsal and volar hand including hypothenar eminence, fifth digit, and ulnar/medial aspect of ring finger
For major injuries to the hand, such as firework blast injuries, all three forearm nerves can be blocked. For injuries to the radial aspect of the hand or the first four digits, consider blocking the median and/or radial nerve(s). For injuries to the ulnar hand or little finger (eg, a boxer’s fracture), utilize the ulnar nerve block. (See Figure 2.) There’s moderate overlap of innervation for each dermatomal location. Injuries located close to dermatomal transitions often require both nerves to be blocked to ensure adequate pain control. We also recommend using a multimodal approach to pain management that relies on oral agents as well as local anesthetic infiltration, if possible.
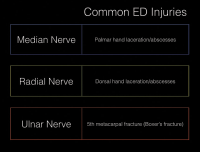
Figure 2. Choosing the correct nerve block for the injured area.
While forearm nerve blocks provide excellent anesthesia for hand injuries (fractures, dislocations, lacerations, abscesses), they don’t provide anesthesia to the volar forearm or the wrist. Therefore, other means of analgesia/anesthesia should be pursued for injuries to these areas, such as distal radius fractures and other wrist injuries.
Ultrasound Setup
Probe: The probe selection should be a high-frequency linear transducer (15-6 MHz) set at the nerve (or soft tissue) preset (found on most POCUS systems). A 10-5 MHz transducer could also be used. Use a standard 1.5-inch, 25-gauge needle. (An alternative is a 22-gauge, blunt-tipped regional block needle.)
Pages: 1 2 3 4 | Single Page



No Responses to “How to Perform Ultrasound-Guided Forearm Nerve Blocks to Provide Non-Drug Pain Relief for Acute Injuries”