
Explore This Issue
ACEP Now: Vol 33 – No 01 – January 2014HOW TO PLACE A BALKEMORE
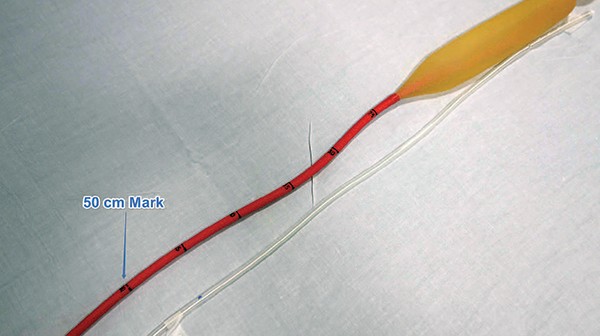
Figure 1. Sengstaken-Blakemore Tube
Figure 2. Christmas tree to male Luer-Lok converter connects Blakemore ports to 3 three-way stopcocks.
Figure 3. Gastric port setup: After placing Blakemore tube, attach Luer-Lok syringe and inflate 50 cc of air. After confirming placement with chest X-ray, inflate an additional 200 cc of air.
Figure 4. Esophageal port setup: Connect one med lock cap to manometer and the other to Luer-Lok syringe. Inflate to 30 mm Hg. If bleeding continues, inflate to 45 mm Hg.
Here’s your shopping list:
- Sengstaken-Blakemore tube
- Salem Sump gastric tube
- 60 mL Luer-Lok syringe
- 60 mL slip-tip syringe
- 2 Christmas tree to male Luer-Lok converters
- 3 three-way stopcocks
- 3 med lock caps
- Surgilube
- Roller bandage (Kling)
- 1 one-liter bag of crystalloid
- May also need: laryngoscope, Magill forceps, hemostat
How to place the tube:
- The patient should be intubated and the head of the bed up at 45 degrees.
- Test balloons on Blakemore and fully deflate. Mark Salem Sump at the 50-cm mark of the Blakemore with the tip 2 cm above gastric balloon and then 2 cm above esophageal balloon.
- Insert the Blakemore tube through the mouth just like an OGT. You may need the aid of the laryngoscope and Magill forceps. Make sure the depth-marker numbers face the patient’s right side.
- Stop at 50 cm. Test with slip-tip syringe while auscultating over stomach and lungs. Inflate gastric port with 50 mL of air.
- Get a chest X-ray to confirm placement of gastric balloon in stomach.
- Once confirmed, inflate with additional 200 mL of air (250 mL total).
- Apply 1 kg of traction using roller bandage and 1 L IV fluid bag hung over an IV pole. Mark the depth at the mouth. The tube will stretch slightly during the next 10 minutes as it warms to body temperature.
- Insert the Salem Sump until the depth-marked gastric is at 50 cm on the Blakemore. Suction both Blakemore lavage port and Salem Sump. You may need to wash blood clots out of the stomach with sterile water or saline.
- If bleeding continues, you will need to inflate esophageal balloon:
- Pull the Salem Sump back until the esoph mark is at the 50 cm point of the Blakemore. Attach a manometer to the second three-way stopcock on the esophageal port of the Blakemore. Inflate to 30 mm Hg. If bleeding continues, inflate to 45 mm Hg.
Conclusion
After you place the Blakemore and inflate the gastric balloon, the bleeding stops and the patient stabilizes. GI arrives and must remove the Blakemore for scope. As soon as it is removed, blood begins gushing into the esophagus. GI is unable to stop the bleeding via EGD, so you are forced to reintroduce the Blakemore. You call IR in, and they take the patient for a TIPS (transjugular intrahepatic portosystemic shunt) procedure, which finally stops the bleeding. Thanks to your efforts, the patient is able to walk out of the hospital after a short ICU stay and eventually has a successful liver transplant.
Pages: 1 2 3 | Single Page


No Responses to “How To Place A Blakemore Tube in an ED Patient with Upper GI Bleeding from Esophageal Varices”