It’s 4 a.m., and you’re three hours from the nearest tertiary care center. A young woman, 13 days post-tonsillectomy, comes into your rural emergency department (ED) coughing up blood. On exam, you see bright red blood trickling down her left tonsillar fossa. Her vital signs are normal, except for a heart rate of 115 bpm. It’s going to take time to get her to a tertiary center.
Explore This Issue
ACEP Now: Vol 44 – No 01 – January 2025Managing post-tonsillectomy hemorrhage in the ED can be challenging, especially in rural or resource-limited settings. The key is a stepwise, three-pronged approach—resuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleeding—to keep the patient safe until she’s transferred to definitive care. Additionally, one must be prepared for definitive airway management and know when laboratory investigations will prove valuable to guide further management. By learning a simple approach, you will be better prepared for the next post-tonsillectomy bleed that rolls through your ED doors.
Know What You’re Dealing With
Understanding the distinction between primary and secondary post-tonsillectomy hemorrhage is fundamental to management and prognostication. Primary hemorrhage occurs within 24 hours after surgery, typically from surgical technique issues or an undiagnosed bleeding disorder, such as von Willebrand disease.
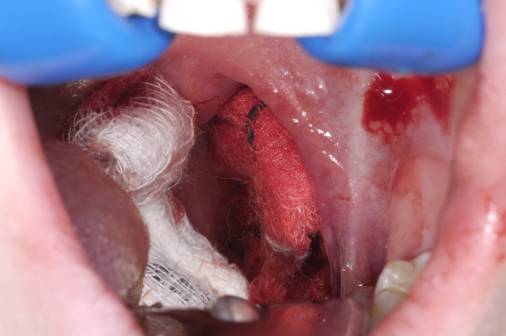
A patient’s mouth packed with gauze after tonsillectomy surgery. CREDIT: Dr. P. Marazzi – Science Source (Click to enlarge.)
Secondary hemorrhage occurs between days five and 14 post-operatively, peaking around days five to seven.1 Secondary bleeds occur because the fibrin clot sloughs off, exposing underlying tissue. Secondary bleeds, often characterized by low-volume bleeding initially—like in this case—can be deceptive but can suddenly increase, causing airway compromise. With any secondary bleed, always keep in mind the “herald bleed” concept. A small trickle from a secondary bleed can be a warning sign for a significant bleed to come, akin to a sentinel bleed from a cerebral aneurysm prior to a large subarachnoid hemorrhage.
Early intervention for all post-tonsillectomy bleeds, whether primary or secondary, is recommended to prevent progression.2 Recognizing secondary hemorrhage and initiating early ENT consultation for potential surgical source control is essential, even if bleeding initially appears mild.3
A three-pronged management approach provides a framework for addressing post-tonsillectomy bleeds: resuscitation, early ENT consultation with transport arrangements, and temporizing measures applied to control bleeding.
Resuscitation
Begin by positioning the patient upright in their position of comfort to reduce the risk for aspiration and improve visualization of the bleeding site. Obtain IV access as soon as possible and consider intravenous (IV) tranexamic acid (TXA), which may help stabilize the clot and buy you time. Although evidence for TXA in post-tonsillectomy bleeds remains limited, studies in postsurgical hemorrhage in general have suggested it is a reasonable intervention with a low risk of adverse effects.4
Pages: 1 2 3 4 | Single Page



3 Responses to “Post-Tonsillectomy Hemorrhage: A Three-Pronged Approach”
January 15, 2025
Creed MamikunianAs an ENT who has practiced for 35 years, I usually managed these patients in the ER awake. Spray topical lidocaine on the side bleeding. Then inject about 2-3 cc 1% lidocaine with epi at the site of bleeding. You need a strong headlight from the OR and a suction bovie machine also from the OR. Have your ENT teach you how to use these various instruments, they are your friend. Calmly talk the patient through what you’re doing and then cauterize the bleeding vessel. It’s usually at the plica triangularis (the bottom of the tonsillar fossa. Use two tongue blades to push the tongue down to find the bleeder. Give it a few good buzzes with the suction bovie and you’re done.
Everything else is just delaying the treatment. One last thing, if it’s a young patient, this won’t work. Teenagers at a minimum. Otherwise, you’d better hope your ENT is close by.
January 19, 2025
Paul MMany of us live in a world where there is no ENT…either on call or close by. Top 5 bad cases at 0300….tonsillar bleed in pediatric patient.
February 20, 2025
Dr James C MartinHaving practiced ENT for 35+ yrs, I’ve seen my share of post-tonsil bleeds, usually 5-10 days postop, but have seen them as late as several weeks. I don’t hesitate to take these patients to the OR, not only for excellent visualization, but there’s nothing worse than stopping the bleeding in the ER, only to be called back 2-3 hrs later because the patient rebled, usually secondary to N/V at home despite anti nausea meds.
Usually cautery or coblation solves the problem, and I then inject 1-2cc of 1/4% marcaine with 1/200K epinephrine for pain control, along with hemostatic effect.
Postop tonsil bleeds can be severe and cause you to age faster, and loose sleep!