Case Resolution
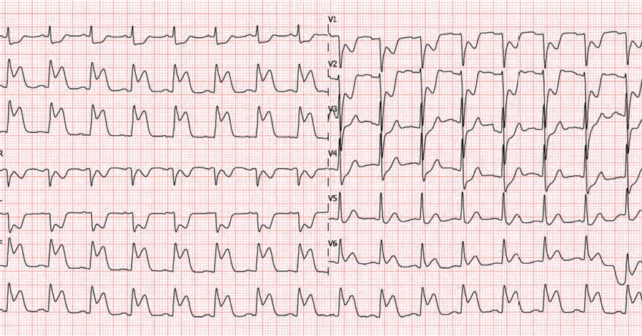
The patient is having eight out of 10 chest pain and the ECG suggests an inferior MI with possible right ventricular involvement. You know the latest evidence doesn’t support the contraindication of nitroglycerin administration and that it might ease his pain. At the same time, you know that any patient with an MI might become hypotensive, so before providing the first spray of nitroglycerin you establish an intravenous line.
Explore This Issue
ACEP Now: Vol 43 – No 03 – March 2024Thank you to Dr. Rupinder Sahsi who works as an emergency physician in Kitchener-Waterloo, Ontario, Canada and is an assistant medical director for EMS at the Centre for Paramedic Education and Research in Hamilton, Ontario, Canada for his assistance with this critical appraisal.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
References
- Neumar RW, Shuster M, Callaway CW, et al. Part 1: Executive summary. Circulation. 2015;132:S315–67.
- Ferguson JJ, Diver DJ, Boldt M, et al. Significance of nitroglycerin-induced hypotension with inferior wall acute myocardial infarction. Am J Cardiol.1989;64:311–4.
- Robichaud L, Ross D, Proulx M-H, et al. Prehospital nitroglycerin safety in inferior ST-elevation myocardial infarction. Prehosp Emerg Care. 2016;20:76–81
- McConnell AH, Davis M, Van Aarsen K, et al. LO33: prehospital adverse events associated with nitroglycerin use in STEMI patients with right ventricle infarction. CJEM. 2017;19:S39.
Pages: 1 2 3 | Single Page



2 Responses to “Revisiting Nitroglycerin in MI with Right-Side Ventricular Involvement”
March 10, 2024
Joseph Shiber, MDYou have missed the big picture. NTG will cause venodilation in every patient. If they are dependent on RV filling for contraction as during myocardial ischemia/infarction then you will expect this effect to be pronounced. It’s not that you can’t give NTG for the anti-anginal effect of potentially pain relief (that’s all the benefit you will ever get from NTG unless there is actual coronary artery spasm w/o complete coronary occlusion/thrombosis) but you need to be ready to intervene by stopping the NTG (it should be IV and not SL or topical since you need the effect to go away quickly) and give an IVF bolus. If you give a SL NTG and do not have IV access yet to give an IVF bolus, you will never forget this mistake even if the patient hopefully doesn’t arrest.
March 10, 2024
Andrew SchareAnother question to ask is why do we give nitrates at all to patients with acute myocardial infarction. There is no benefit to morbidity or mortality.