
Explore This Issue
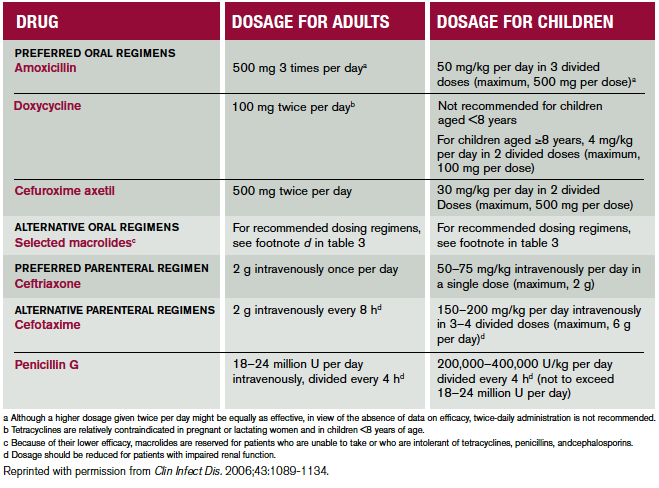
ACEP Now: Vol 33 – No 08 – August 2014Table 1. Recommended Antimicrobial Regimens for Treatment of Patients With Lyme Disease.The management options considered included oral antimicrobial therapy for patients with a single erythema migrans skin lesion and oral versus parenteral therapy for patients with clinical evidence of early disseminated infection (ie, patients presenting with multiple erythema migrans lesions, carditis, cranial nerve palsy, meningitis, or acute radiculopathy).
While Lyme carditis is an uncommon manifestation of Lyme disease, it is also one of the most serious. Emergency health care providers are in a unique position to recognize and diagnose this potentially life-threatening illness before it progresses. Additional information about the prevention, diagnosis, treatment, and epidemiology of Lyme disease can be found at www.cdc.gov/lyme.
Acknowledgements
The author would like to thank the coauthors of the Morbidity and Mortality Weekly Report describing this investigation:1 Gregory Ray, MD, Thadeus Schulz, MD, Wayne Daniels, DO, Cryolife, Inc., Kennesaw, Georgia; Elizabeth R. Daly, MPH, New Hampshire Department of Health and Human Services; Thomas A. Andrew, MD, New Hampshire Office of the Chief Medical Examiner; Catherine M. Brown, DVM, Massachusetts Department of Public Health; Peter Cummings, MD, Massachusetts Office of the Chief Medical Examiner; Randall Nelson, DVM, Matthew L. Cartter, MD, Connecticut Department of Public Health; P. Bryon Backenson, MS, Jennifer L. White, MPH, Philip M. Kurpiel, MPH, Russell Rockwell, PhD, New York State Department of Health; Andrew S. Rotans, MPH, Christen Hertzog, Linda S. Squires, Dutchess County Department of Health, New York; Jeanne V. Linden, MD, Wadsworth Center, New York State Department of Health; Margaret Prial, MD, Orange County Office of the Medical Examiner, New York; Jennifer House, DVM, Pam Pontones, MA, Indiana State Department of Health; Brigid Batten, MPH, Dianna Blau, DVM, PhD, Marlene DeLeon-Carnes, Atis Muehlenbachs, MD, PhD, Jana Ritter, DVM, Jeanine Sanders, Sherif R. Zaki, MD, PhD, Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Disease; Paul Mead, MD, Alison Hinckley, PhD, Christina Nelson, MD, Anna Perea, MSc, Martin Schriefer, PhD, Claudia Molins, PhD, Division of Vector-Borne Diseases, National Center for Emerging and Zoonotic Infectious Disease.
When to Provide Prophylaxis
For prevention of Lyme disease after a recognized tick bite, routine use of antimicrobial prophylaxis or serologic testing is not recommended. A single dose of doxycycline may be offered to adult patients (200 mg) and to children ≥8 years of age (4 mg/kg, up to a maximum dose of 200 mg) when all of the following circumstances exist:
- The attached tick can be reliably identified as an adult or nymphal I. scapularis tick that is estimated to have been attached for ≥36 hours on the basis of the degree of engorgement of the tick with blood or on certainty about the time of exposure to the tick.
- Prophylaxis can be started within 72 hours of the time that the tick was removed.
- Ecologic information indicates that the local rate of infection of these ticks with B. burgdorferi is ≥20 percent.
- Doxycycline is not contraindicated.
Source: Clin Infect Dis. 2006;43:1089-1134.
Pages: 1 2 3 4 | Single Page




No Responses to “Risk of Sudden Cardiac Arrest from Lyme Carditis Underscores Need for Timely Diagnosis, Treatment”