The Case
Anna comes to your emergency department after her boyfriend hit her several times in the face before strangling her, resulting in her losing consciousness. She has marked facial ecchymosis and swelling especially to her right orbit and cheek. There are no facial petechiae noted, but there are small bilateral subconjunctival hemorrhages present. Her neck reveals linear bruising on the right side; the remainder of her physical exam is normal. The emergency department team evaluates and treats her injuries.
Explore This Issue
ACEP Now: Vol 37 – No 08 – August 2018Initially, Anna declines police notification, and her state’s laws prohibit notification of law enforcement without patient consent. The emergency department team arranges for a social worker to meet with Anna. As part of this consult, the social worker uses the Danger Assessment (DA) tool and finds her level of danger extreme. Armed with this information, the social worker counsels Anna and contacts the local domestic violence hotline, which arranges for a crisis counselor to come to the hospital to talk to Anna. With Anna’s permission, police are notified. The agency helps her secure a legal protective order with law enforcement and assists her with seeking safe housing upon hospital discharge.
Danger Assessment Tool
The DA is a tool used to estimate the risk of being killed by an intimate partner (IP) in a violent intimate relationship. It consists of a calendar to assess the frequency and severity of incidences of abuse and 20 yes-or-no questions. The results of the 20-question portion are categorized as:
- <8: Variable danger
- 8–13: Increased danger
- 14–17: Severe danger
- >18: Extreme danger
Recent modifications of the DA include versions for same-sex relationships and immigrants and a simplified five-item version.
Why is the DA important? Every year, 1,500 to 1,600 women are killed by an IP, accounting for 40 percent to 50 percent of all femicides in the United States. Approximately 67 percent to 80 percent of IP homicides involve a history of physical abuse prior to the murder. Use of the DA can help identify those at greatest risk for homicide.
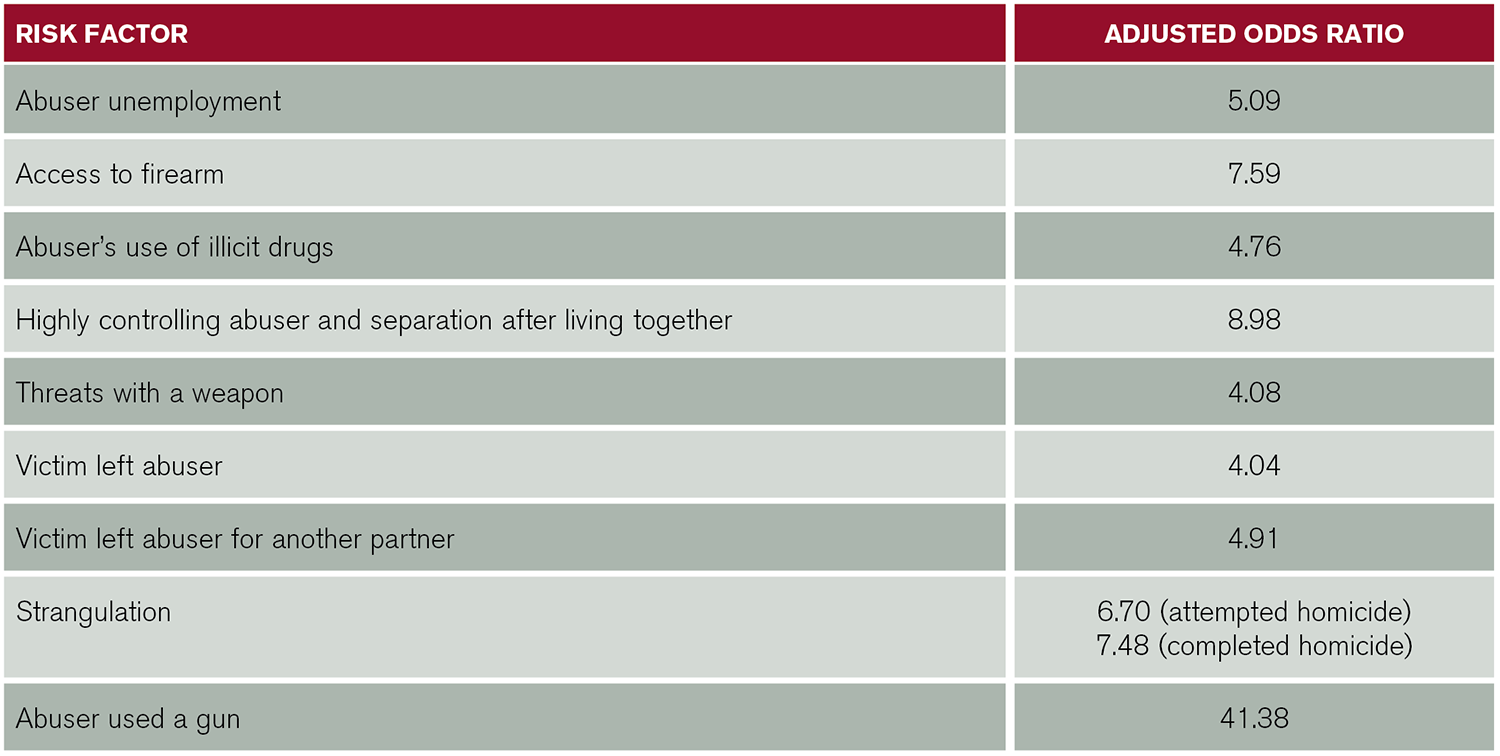
(click for larger image) Table 1: Factors Associated with a Higher Risk for Intimate Partner Homicide
Source: Am J Public Health. 2003;93(7):1089-1097.
We recommend the DA for all emergency department patients following IP violence (IPV). Hospitals should have 24-7 access to a social worker or a representative from the local IPV advocacy center to come to the emergency department, administer the assessment, and provide the patient with safety-planning options. Telephonic advocate consultation and/or emergency department staff administration of shorter versions of the DA may also be reasonable options.
The emergency department staff should know how to access the available resources to help victims of IPV and how to assess patients for danger (see Table 1). All of us who care for IPV victims must anticipate their needs beyond emergency department care (DA). The consequences of not knowing their level of risk can be lethal.
Resources for Further Reading
- Campbell JC, Webster D, Koziol-McLain J, et al. Risk factors for femicide in abusive relationships: results from a multisite case control study. Am J Public Health. 2003;93(7):1089-1097.
- Glass N, Perrin N, Hanson G, et al. Risk for reassault in abusive female same-sex relationships. Am J Public Health. 2008;98(6):1021-1027.
- Messing JT, Amanor-Boadu Y, Cavanaugh CE, et al. Culturally competent intimate partner violence risk assessment: adapting the Danger Assessment for immigrant women. Soc Work Res. 2013;37(3):263-275.
- Snider C, Webster D, O’Sullivan C, et al. Intimate partner violence: development of a brief risk assessment for the emergency department. Acad Emerg Med. 2009;16(11):1208-1216.
Pages: 1 2 | Multi-Page



No Responses to “The Danger Assessment Tool Determines Patients’ Risk of Domestic Abuse”