
Case 1
A 39-year-old female is transferred to your emergency department from an outpatient same-day surgery center. The patient reportedly developed tachycardia and tachypnea while in the postoperative suite approximately 30 minutes after undergoing general anesthesia for a colonoscopy. She was sent to your emergency department for evaluation, where she was found to be hyperthermic with a rectal temperature of 106.5ºF. You notice a rising end-tidal CO2 despite no change in ventilation and severe masseter muscle spasm.
Explore This Issue
ACEP Now: Vol 35 – No 12 – December 2016Case 2
A 73-year-old male with a past medical history of Parkinson’s disease presents to the emergency department from home with fever and altered mental status. His vital signs are blood pressure 98/59, pulse 102, respiration 15, and temperature 102.6ºF. On exam, you recognize “lead pipe” rigidity and bradykinesia. A septic workup is performed, but there is no obvious source of infection. His wife reports he stopped taking his “Parkinson’s medication” a few days ago.
Case 3
A 27-year-old male with a past medical history of depression, currently treated with fluoxetine, is brought into the emergency department by his girlfriend for altered mental status. He is febrile with a temperature of 102.2ºF, but the rest of his vital signs are within normal limits. He is agitated, is diaphoretic, and has lower extremity clonus. His girlfriend shows you a bottle of dextromethorphan and reports the patient started taking it yesterday for a cough.
The cases above describe three different hyperthermic disorders: malignant hyperthermia, neuroleptic malignant syndrome (NMS), and serotonin syndrome. These syndromes are often confused with one another when being considered in the diagnosis of a hot and stiff patient presenting to the emergency department (see Table 1).
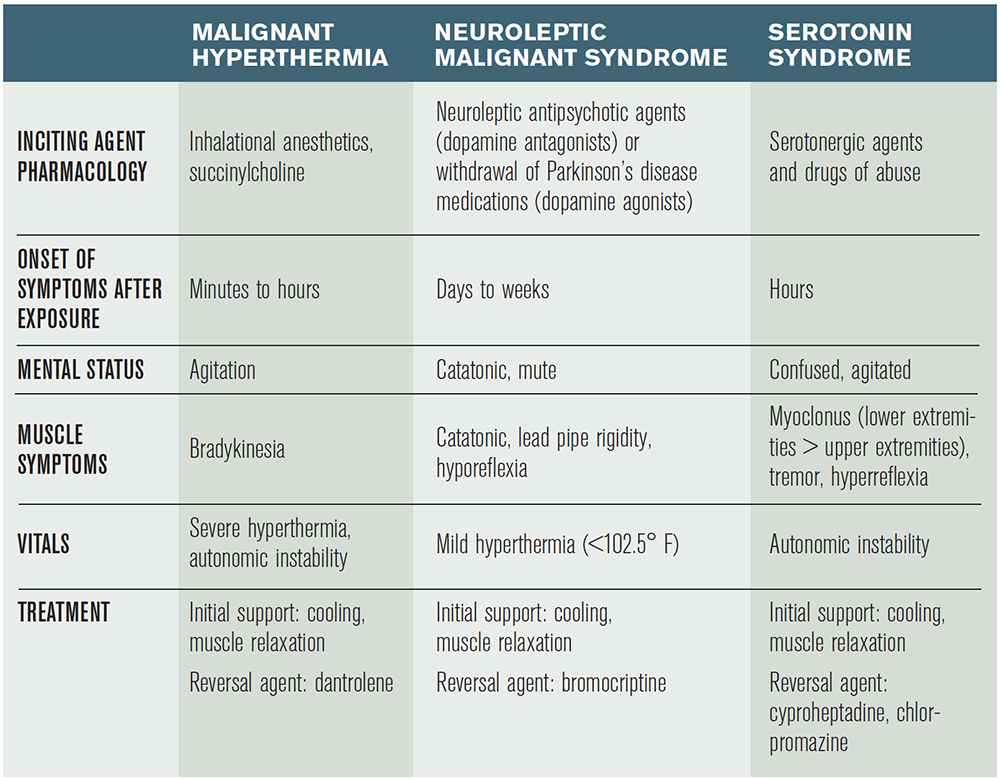
(click for larger image) Table 1. Management of Toxin-Induced Hyperthermic Disorders
Malignant Hyperthermia
Malignant hyperthermia is a hypermetabolic syndrome of skeletal muscle, which can occur in individuals with inherited defects of their ryanodine L-type calcium channels. These calcium-release channels are located in the sarcoplasmic reticulum of skeletal muscle and dump out large quantities of calcium ions when stimulated by exposure to certain agents.1 The increase in intracellular calcium levels in skeletal muscle causes increased muscle contraction and increased consumption of adenosine triphosphate, releasing excessive heat, resulting in hyperthermia. The most common agents responsible for causing malignant hyperthermia are certain volatile gas anesthetics (halothane, sevoflurane, desflurane) and succinylcholine. There have also been case reports of excessive exercise and heat leading to the condition.2
Pages: 1 2 3 4 | Single Page



No Responses to “Tips for Diagnosing,Treating Toxin-Induced Hyperthermic Disorders”