
Explore This Issue
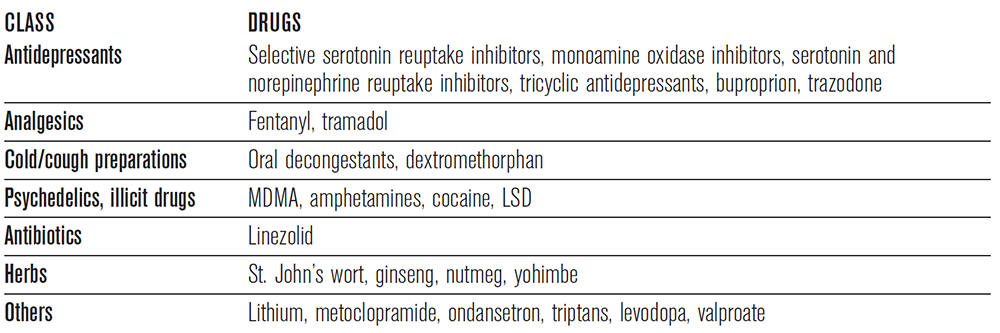
ACEP Now: Vol 35 – No 12 – December 2016(click for large image) Table 2: Drugs That May Cause Serotonin Syndrome
The symptoms of serotonin syndrome are extremely variable, ranging from mild presentations to a life-threatening syndrome. The most common presenting symptoms are muscle rigidity, altered mental status, and hyperthermia. Classically, and differentiating this condition from the other hyperthermic disorders, patients develop myoclonus, which is characteristically more evident in the lower extremities. The onset of symptoms is typically rapid, with symptoms typically presenting within minutes to hours. The cornerstone to management of serotonin syndrome involves immediate discontinuation of all serotonergic agents as well as supportive treatment with aggressive cooling and benzodiazepines. Current recommendations include the use of cyproheptadine, an antihistamine with antiserotonergic properties, and chlorpromazine, a phenothiazine antipsychotic with antiserotonergic properties.10 Mortality rates are similar to that of NMS, between 2 and 12 percent.
Treatment
Management of patients with the described toxin-induced hyperthermic disorders begins with supportive care and focuses on decreasing muscle activity (benzos) and core body temperature (and chill). Benzodiazepines play an important role in decreasing mortality by reducing shivering and muscle breakdown that can lead to rhabdomyolysis, hyperkalemia, and ultimately renal failure. Patients with severe toxicity who do not respond to benzodiazepines may even require chemical paralysis with a non-depolarizing paralytic agent along with mechanical ventilation for better control of their muscle hyperactivity.
Dr. Traficante is a PGY-3 resident and Dr. Kashani is a physician in the department of emergency medicine at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
References
- MacLennan DH. The genetic basis of malignant hyperthermia. Trends Pharmacol Sci. 1992;13(8):330-334.
- Rosenberg H, Davis M, James D, et al. Malignant hyperthermia. Orphanet J Rare Dis. 2007;2:21.
- Larach MG, Gronert GA, Allen GC, et al. Clinical presentation, treatment, and complications of malignant hyperthermia in North America from 1987 to 2006. Anesth Analg. 2010;110(2):498-507.
- Britt BA, Kalow W. Malignant hyperthermia: a statistical review. Can Anaesth Soc J. 1970;17:293-315.
- Gurrera RJ, Caroff SN, Cohen A, et al. An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method. J Clin Psychiatry. 2011;72(9):1222-1228.
- Gurrera RJ. Sympathoadrenal hyperactivity and the etiology of neuroleptic malignant syndrome. Am J Psychiatry. 1999;156(2):169-180.
- Modi S, Dharaiya D, Schultz L, et al. Neuroleptic malignant syndrome: complications, outcomes, and mortality. Neurocrit Care. 2016;24(1):97-103.
- Strawn JR, Keck PE Jr, Caroff SN. Neuroleptic malignant syndrome. Am J Psychiatry. 2007;164(6):870-876.
- Buckley NA, Dawson AH, Isbister GK. Serotonin syndrome. BMJ. 2014;348:g1626.
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352:1112-1120. Erratum in: N Engl J Med. 2007;356:2437.
Pages: 1 2 3 4 | Single Page




No Responses to “Tips for Diagnosing,Treating Toxin-Induced Hyperthermic Disorders”