Pain management of the acutely injured patient with rib fractures can be difficult for even the most experienced emergency physician. Severe pain from multiple rib fractures (or even one) can impair ventilatory function, decreasing the ability to clear respiratory secretions and increasing rates of nosocomial pneumonias.1,2 A multimodal approach to pain control via intravenous medications (eg, opioids, ketamine, acetaminophen, etc.) is reasonable but often insufficient. Epidural analgesia, recommended strongly by trauma guidelines for patients with multiple rib fractures, is often not acutely available in the emergency department. An opioid-sparing multimodal approach that integrates regional anesthesia is believed to be optimal for patients.3 Alternatives such as intercostal blocks are time-intensive, involve multiple injections, are often more difficult to perform, and necessitate patient repositioning.4 The ultrasound-guided serratus anterior plane block (SAPB) is a promising single-injection method to anesthetize the chest wall in patients with multiple rib fractures, providing optimal emergency department care.1
Explore This Issue
ACEP Now: Vol 36 – No 03 – March 2017Anatomy and Innervation
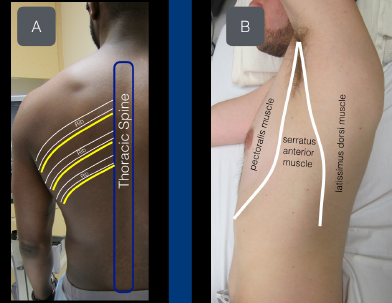
Figure 1A: View of the thoracic intercostal nerves as they exit the spine inferior to the ribs.
Figure 1B: The serratus anterior muscle sits between the pectoralis muscle (anterior) and latissimus dorsi muscle (posterior).
The chest wall is innervated from the lateral cutaneous branches of the thoracic intercostal nerves (T2–T12). The thoracic intercostal nerves run with the intercostal artery and vein, just under the rib, traveling in an anterolateral direction. As the thoracic intercostal nerve reaches the midaxillary line, the lateral cutaneous branch of the intercostal nerve pierces the internal intercostal muscle, external intercostal muscle, and serratus anterior muscle to innervate the musculature of the thorax. The serratus anterior muscle is a

Figure 2: Schematic representation of the intercostal nerves as they travel from the thoracic spine. The distal lateral cutaneous branch exits at approximately the midaxillary line and pierces the internal intercostal muscle, external intercostal muscle, and serratus anterior muscle. The anterior fascial plane above the serratus anterior muscle acts as the target for this planar block.
readily visualized sonographic landmark, located posterior to the lateral edge of the pectoralis muscle and anterior to the lateral edge of the latissimus dorsi muscle (see Figures 1A and 1B). The distal branches of the thoracic intercostal nerves (lateral cutaneous intercostal nerves) provide innervation to the lateral thoracic cage and lie in the fascial plane just superficial to the serratus anterior muscle (see Figure 2). Placing large-volume dilute anesthetic solution into this potential space (formed by the serratus anterior muscle) is theorized to spread in a cephalad and caudal direction with patient respirations, providing analgesia for thoracic injuries (and specifically rib fractures).5
Supplies
- High-frequency linear transducer (13–6 MHz)
- Anesthetic: 15 mL bupivacaine 0.5% (5 mg/mL; maximum 2 mg/kg) and 15 mL normal saline placed in a 30 mL syringe (note: in patients under 40 kg, please be aware of the need to lower the volume of anesthetic)
- 22 g blunt-tip block needle or 20–22 g Quincke spinal needle
- 91 cm or 36″ tubing (or similar tubing)
- Cleaning solution
- 25–30 g needle for local skin wheal
Because of the large volume of dilute anesthetic planned to be deposited in the fascial plane above the serratus anterior muscle, we recommend a two-provider technique. In a 30 mL syringe, place a mixture of 15 mL 0.5% bupivacaine and 15 mL normal saline. Connect the needle to the tubing and prime the circuit to ensure all air is removed.
Procedure
1. Pre-block.
Pages: 1 2 3 4 | Single Page




6 Responses to “Ultrasound-Guided Serratus Anterior Plane Block Can Help Avoid Opioid Use for Patients with Rib Fractures”
April 3, 2018
Santi Di PietroCongratulations for the article! Clear and complete… how should I cite it in a scientific research?
Sincerely
Santi Di Pietro
Junior EM Resident,
University of Pavia
April 9, 2018
Dawn Antoline-WangThe citation for this article is:
Nagdev A, Mantuani D, Durant E, Herring A. The ultrasound-guided serratus anterior plane block. ACEP Now. 2017;36(3):12-13.
August 14, 2018
Jonathan CheungIs this plane block effective as a one-off procedure or do you often need to repeat it later?
May 9, 2020
Dr.S.RadhakrishnaThank you for this useful article. The figure 2 shows the vertebra pointing in the wrong direction. The spinous process should point posteriorly and the body anteriorly. An error?
March 23, 2021
Dr Maya DehranThanks for sharing the very useful simple technique to treat the severe pain of chest injury.
January 18, 2022
DAVID CAMPELL, MDHow long does this block last before it has to be repeated to maintain pain control?