4. Antibiotics
Explore This Issue
ACEP Now: Vol 43 – No 06 – June 2024Empiric broad-spectrum antibiotic regimens in the acute stages of severe sepsis and septic shock are becoming a mainstay of treatment. The SSC guidelines base antimicrobial administration recommendations on the following: likelihood of a current infectious process based on clinical examination, suspicion for MRSA or MDR organisms, and viral or fungal sources.7 MRSA nasal swabs, when negative, can eliminate the need for MRSA coverage in sepsis patients.5 There is no current recommendation for a specific antibiotic regimen, but administration of broad-spectrum coverage must be completed within one hour of recognizing septic shock (strong recommendation) or within three hours of recognizing sepsis without shock.5 Each institution will have its own unique microbiome, but, as an example, a suggested antibiotic regimen is presented in tabular form based on Michigan Medicine’s recommendations (Table 2).5 Ferrer and colleagues investigated time to antibiotic administration in severe sepsis and septic shock, concluding that for every hour a physician delays antibiotic coverage, there was a statistically significant increase in mortality.12 Another retrospective cohort study investigated the association between door-to-antibiotic time of patients with clinical sepsis and longterm mortality. Their median door-to-antibiotic time averaged 166 minutes, leading to a one-year mortality risk of 19 percent. Each additional hour delay in antibiotic administration was associated with 10 percent increased odds of one-year mortality.13
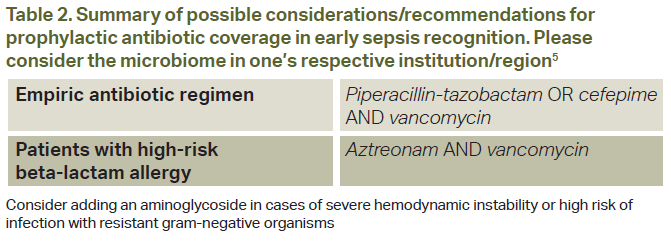
Click to enlarge.
In summary, the current recommendations for antibiotic coverage are based on suspicion for an acute bacterial process, and administration of a “broad” antimicrobial regimen is recommended within one hour of recognizing septic shock or within three hours in sepsis without shock.
5. Vasopressors
Current recommendations by the SSC follow a stepwise pattern when considering vasopressor therapy after adequate volume resuscitation. The first recommendation is the use of norepinephrine, followed by vasopressin and then epinephrine if a MAP >65 mmHg cannot be obtained. If there is cardiac dysfunction, one may add dobutamine to supplement norepinephrine or utilize epinephrine alone.7 It is important to mention that both the CENSER and CLOVERS trials investigated standard sepsis management (intravenous fluids followed by vasopressors) versus the early use of norepinephrine. CENSER determined that early norepinephrine use was associated with increased shock control by six hours compared to standard therapy, and CLOVERS concluded that mortality and adverse events were similar between the two groups.11,14 For adults with septic shock on norepinephrine with inadequate MAP levels (<65 mmHg), vasopressin is recommended rather than escalating doses of norepinephrine.5



One Response to “Updates in the Management of Severe Sepsis and Septic Shock”
July 1, 2024
Joseph R Shiber, MDDear ACEPNow Editor,
Excellent synopsis of ED treatment of septic shock but I would like to add a few clarifications. The preferred balanced IVF is Plasmalyte-A since LR is somewhat hypotonic (Na 130) and uses lactate as a buffer, compared to acetate and gluconate in Plasmalyte-A (Na 140). The additional lactate is not actually detrimental to cellular activity but can hamper the usefulness of tracking lactate levels especially with hepatic or mitochondrial dysfunction where lactate is not being converted back to pyruvate for preparation to enter the TCA cycle. The optimal vasopressor for septic shock should correct the hemodynamic disorder(s) causing the tissue hypoxia. Levophed is certainly the most useful to help restore vascular tone (alpha effect) in the low SVR vasodilatory state of distributive shock while supplying a small B1-2 effect but there are cases where an inappropriate heart-rate response occurs (HR <80) due to medications (such as AVN blockers) or to intrinsic chronotropic failure (age or sepsis related). In these cases, it is paramount to address the heart rate at the same time, since if the heart rate remains inappropriately low while simply increasing SVR the cardiac output and tissue perfusion will potentially go down not up. Lastly, although ECMO is well recognized as a rescue for ARDS (V-V) and circulatory shock (V-A) it should be noted that active bacteremia or fungemia is a contraindication since the circuit will be contaminated immediately and cannot be sterilized.
Respectfully,
Joseph Shiber, MD, FACEP, FACP, FNCS, FCCM