Explore This Issue
ACEP Now: Vol 35 – No 12 – December 2016Conclusion
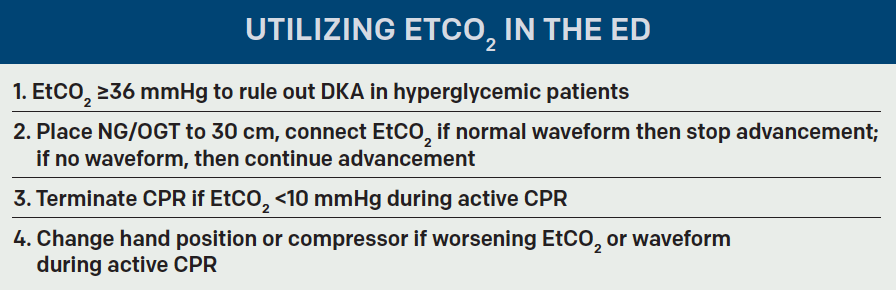
End-tidal capnometry wasn’t meant to be kept in the stable and only used for the occasional procedural sedation. Try taking it out for a ride on your next shift, whether it’s for screening the next hyperglycemic patient for diabetic ketoacidosis, monitoring for disposition of a wheezing asthmatic, resuscitating or terminating an active cardiac arrest, or confirming placement of an NGT. Remember to use caution in patients with underlying lung disease such as chronic obstructive pulmonary disease. Throughout each shift, emergency physicians make critical decisions by pooling myriad data points from the history, physical exam, labs, imaging studies, and many other variables that we may subconsciously consider. End-tidal capnometry provides us with another data point that can aid in these crucial choices and requires few resources, money, or time.
 Dr. D’Amore is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
Dr. D’Amore is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
 Dr. McNamee is an attending physician at Emergency Medicine Professionals in Ormond Beach, Florida.
Dr. McNamee is an attending physician at Emergency Medicine Professionals in Ormond Beach, Florida.
 Dr. McGovern is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
Dr. McGovern is an emergency medicine resident at St. Joseph’s Regional Medical Center in Paterson, New Jersey.
References
- Weinberg L, Skewes D. Pneumothorax from intrapleural placement of a nasogastric tube. Anaesth Intensive Care. 2006;34(2):432-436.
- Woodall BH, Winfield DF, Bisset GS 3rd. Inadvertent tracheobronchial placement of feeding tubes. Radiology. 1987;165:727-729.
- Stroud M, Duncan H, Nightingale J, et al. British Society of B. Guidelines for enteral feeding in adult hospital patients. Gut. 2003;52(supp 7):vii1-vii12.
- Meyer P, Henry M, Maury E, et al. Colorimetric capnography to ensure correct nasogastric tube position. J Crit Care. 2009;24:231-235.
- Jolliet P, Pichard C, Biolo G, et al. Enteral nutrition in intensive care patients: a practical approach. Working Group on Nutrition and Metabolism, ESICM. European Society of Intensive Care Medicine. Intensive Care Med. 1998;24:848-859.
- Chau JP, Lo SH, Thompson DR, et al. Use of end-tidal carbon dioxide detection to determine correct placement of nasogastric tube: a meta-analysis. Int J Nurs Stud. 2011;48:513-521.
- Neumar RW, Otto CW, Link MS, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S729-767.
- Kalenda Z. The capnogram as a guide to the efficacy of cardiac massage. Resuscitation. 1978;6(4):259-263.
- Idris AH, Staples ED, O’Brien DJ, et al. End-tidal carbon dioxide during extremely low cardiac output. Ann Emerg Med. 1994;23:568-572.
- Sheak KR, Wiebe DJ, Leary M, et al. Quantitative relationship between end-tidal carbon dioxide and CPR quality during both in-hospital and out-of-hospital cardiac arrest. Resuscitation. 2015;89:149-154.
- Institute of Medicine. Strategies to improve cardiac arrest survival: a time to act. Washington, DC: The National Academies Press; 2015.
- Kolar M, Krizmaric M, Klemen P, et al. Partial pressure of end-tidal carbon dioxide successful predicts cardiopulmonary resuscitation in the field: a prospective observational study. Crit Care. 2008;12(5):R115.
- Poon KM, Lui CT, Tsui KL. Prognostication of out-of-hospital cardiac arrest patients by 3-min end-tidal capnometry level in the emergency department. Resuscitation. 2016;102:80-84.
- Deakin CD, Morrison LJ, Morley PT, et al. Part 8: advanced life support: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2010;81(Suppl 1):e93-e174.
- TLui CT, Poon KM, Tsui KL. Abrupt rise of end tidal carbon dioxide level was a specific but non-sensitive maker of return of spontaneous circulation in patient with out-of-hospital cardiac arrest. Resuscitation. 2016;104:53-58.
Pages: 1 2 3 4 | Single Page




No Responses to “Use End-Tidal Capnography for Placing Orogastric, Nasogastric Tubes, and CPR”