The Case
A 25-year-old man with no past medical history presented to the emergency department with bilateral hand pain. This was his third ED presentation. During his second visit, at an outside facility, he was diagnosed with cellulitis and prescribed doxycycline. Despite taking antibiotics for two days, the pain and swelling continued to worsen, particularly in the left third digit. Symptoms initially began six days prior to presentation, when he noticed a small, raised lesion to the palm of his right hand. Several days later, he observed swelling and redness to the dorsum of his left hand and middle finger. He also began having pain in his right thumb while reporting decreased range of motion in both wrists and hands. The patient reported having subjective fever five days prior and left knee pain two days prior. He denied history of trauma. The patient worked as a waiter in a restaurant and had no history of IV drug use but acknowledged intermittent use of cocaine and alcohol. The patient denied recent unprotected intercourse. He also denied dysuria, penile discharge, or genital lesions.
Explore This Issue
ACEP Now: Vol 40 – No 05 – May 2021Objectively, the patient presented afebrile, with a heart rate of 105 bpm and blood pressure of 139/88. On exam, his left hand had dorsal erythema and edema. His middle finger was held in flexion, swollen, tender to palpation, and painful with passive extension. The patient had limited active range of motion of the left wrist and middle digit with flexion. On the right hand, the patient had a 2 mm brown pustule on his palm. The right thumb was held in flexion with diffuse edema and had limited active range of motion due to pain. His left knee did not have any overlying skin changes or large effusions and had full range of motion without pain.
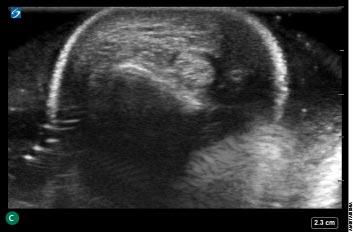
Soft tissue point-of-care ultrasound (POCUS) revealed fluid surrounding the flexor sheath at the left middle finger and also in the right thumb (see Figure 1). Laboratory was notable for a leukocytosis to 18.6, a C-reactive protein of 124.6, and an erythrocyte sedimentation rate of 50. Other basic laboratory results were normal. X-rays of the bilateral hands and left knee were unremarkable. Urine DNA amplification for gonorrhea and chlamydia were sent to lab.

Figure 1: Soft tissue point-of-care ultrasound showing fluid surrounding the flexor sheath at the left middle finger (A) and right thumb (B and C). Credit: Amir Tabibnia

In the emergency department, the patient was given IV fluids and started on vancomycin, piperacillin/tazobactam, and clindamycin. A consultation with hand surgery was initiated. Because the findings were bilateral, the consultants deferred immediate surgery and requested admission to continue IV antibiotics with suspicion of a nonbacterial and, more likely, rheumatologic source. However, because of the POCUS findings, the surgical team evaluated the patient sooner. (Initially, the bilateral nature of the symptoms were seen as inconsistent with a dangerous soft tissue infection.) He was admitted to the inpatient medicine team with the hand surgery following. By this time, the urine gonorrhea resulted as negative.
Rheumatology and infectious disease were consulted and advised to maintain the patient on vancomycin and ceftriaxone, with high suspicion of disseminated gonococcal infection despite a negative urine gonorrhea. On the second day of admission, the patient continued to report persistent pain without improvement, so he was taken to the operating room. The surgery team performed an irrigation and debridement of the left middle finger flexor tendon sheath and irrigation of his flexor tendon sheath of the right thumb with bilateral carpal tunnel releases. Intraoperatively, the patient was found to have extensive purulence of the left hand and middle finger tendon sheath, extending down into the carpal tunnel. He was also found to have a small amount of seropurulent fluid of the right thumb flexor tendon sheath. The postoperative diagnosis was flexor tenosynovitis.
During his stay, the patient had a throat swab that was positive for gonorrhea. The patient then confirmed having oral intercourse with a sex worker. Unfortunately, the operative wound cultures were unable to be tested for gonorrhea or chlamydia, but bacterial cultures had no growth. Blood cultures remained negative, as did HIV and rapid plasma reagin testing. He continued to receive ceftriaxone for presumed disseminated gonococcal infection and was discharged on hospital day seven with an intravenous midline in place to complete a 14-day course of ceftriaxone. The patient had improvement of his infection at his initial follow-up appointment but still had limited range of motion.
Discussion
Flexor tenosynovitis (FTS) is a surgical emergency due to its propensity to cause irreversible damage to tendons, leading to loss of function of the digits and possibly the entire hand.1,2 Clinically, it can present with some or all of the cardinal Kanavel’s signs, including flexed posture of the affected digit, pain on passive extension, tenderness along the flexor sheath, and fusiform swelling.2,3,4
Infectious FTS is usually a direct cause of trauma, commonly puncture wounds or, classically, high-pressure injection injuries from paint solvents.2,4 However, FTS can develop after hematogenous spread from atraumatic sources of infection.2 Often Neisseria gonorrhoeae is the culprit in hematogenous spread and should be suspected in sexually active patients.2,4,5
This patient presented with bilateral FTS likely due to hematogenous spread of a disseminated gonococcal infection from an oral sexual encounter. The triad of disseminated gonococcal infections of tenosynovitis, dermatitis, and arthralgias was present.5,9 The patient also exhibited all four of Kanavel’s cardinal signs, though these physical exam findings are not specific, and they only project higher sensitivity when occurring in combination.4
Despite presenting to two other emergency departments, the patient was presumed to have cellulitis prior to his arrival. Urine studies were negative for gonorrhea and chlamydia, but the patient eventually confirmed positive for gonorrhea on an oral swab. POCUS proved invaluable in quickly elevating clinical suspicion of FTS and in convincing specialists to evaluate the patient promptly. While the POCUS findings did not result in immediate operating room transfer, they did expedite the consultation in the emergency department. This meant that when things worsened later, the team already knew the patient and had been following the course.
Intraoperatively, the patient was found to have purulent findings bilaterally. Generally, suppurative FTS is seen unilaterally and rarely found bilaterally. Disseminated gonococcal infections are also often from a genitourinary source, but this patient was negative for urine gonorrhea. Physicians should consider oral, rectal, cervical, and wound testing as appropriate when there is a high suspicion for a possible gonococcal infection.
Conclusion
Though FTS is usually found unilaterally, physicians should consider disseminated gonorrhea in any patient presenting with possible atraumatic FTS. A complete history should include sexual history, and consider testing oral and rectal sources if urine gonorrhea studies are normal. POCUS is a powerful adjunct and can be especially useful in challenging cases.
Management of FTS includes immediate consultation with hand or plastic surgery for operative consideration, IV antibiotics, and admission.2,3,4
 Dr. Tabibnia is an attending physician in the department of emergency medicine at Cedars-Sinai Medical Center in Los Angeles and assistant clinical professor and ultrasound faculty in the department of emergency medicine at UCLA David Geffen School of Medicine.
Dr. Tabibnia is an attending physician in the department of emergency medicine at Cedars-Sinai Medical Center in Los Angeles and assistant clinical professor and ultrasound faculty in the department of emergency medicine at UCLA David Geffen School of Medicine.
 Dr. Haase is an emergency medicine resident at UCLA David Geffen School of Medicine.
Dr. Haase is an emergency medicine resident at UCLA David Geffen School of Medicine.
How To: POCUS of the Hand with Water Bath
Emergency physicians can adequately identify signs of FTS using bedside ultrasound.6 To obtain the best images possible, it is often easier to perform with a water bath. It is not necessary to apply gel or have direct contact with the patient’s injured and painful extremity.
To perform the water bath technique:
- Use a linear or other high-frequency ultrasound probe.
- Inspect probe, taking extra caution to ensure there are no cracks or open wires to avoid equipment damage.
- Take a basin (big enough for the entire hand to fit) and fill it with tap water.
- Submerge the patient’s hand in the water, with the volar aspect facing up. This is easier because the patient will prefer the hand and digits flexed, and it will also place the point of interest more superficial on the image.
- Place the linear probe into the water and acquire a long axis view with the probe parallel to the digit, no more than a couple of centimeters away from the digit.
- Normal anatomy (superficial to deep) includes epidermis, subcutaneous tissue, flexor tendon, and phalanges (bone presents as hypoechoic [bright] lucency with posterior shadowing).
- Pathological findings include:
- Cobble-stoning, where layered hypoechoic (dark) fluid encircles adipose tissue. Although this is commonly found in cellulitis, this can also be found in FTS but is not diagnostic on its own.
- Anechoic (completely dark) fluid anterior to a flexor tendon and, in more severe cases, circumferentially. This finding is sensitive for FTS.7
- Enlargement of a tendon sheath: Measure the flexor tendon from outer to outer using calipers (see Figure 2). It is considered abnormal if the affected tendon measures 25 percent bigger than the contralateral digit.6,8 This finding is not necessarily needed to make the diagnosis, but if you don’t identify fluid along the tendon sheath and still have high clinical suspicion for FTS, consider this measurement.
- To obtain transverse images, place the point of interest in the middle of the screen and rotate the probe 90 degrees clockwise or counterclockwise.

Figure 2: Long axis view of the finger with hypoechoic fluid superficial to the tendon. The anterior-posterior measurement of the tendon sheath can be compared to the contralateral unaffected hand to support a FTS diagnosis. Credit: Amir Tabibnia
References
- Pang HN, Teoh LC, Yam AKT, et al. Factors affecting the prognosis of pyogenic flexor tenosynovitis. J Bone Joint Surg Am. 2007;89(8):1742-1748.
- Chapman T, Ilyas AM. Pyogenic flexor tenosynovitis: evaluation and treatment strategies. J Hand Microsurg. 2019;11(3):121-126.
- Giladi AM, Malay S, Chung KC. A systematic review of the management of acute pyogenic flexor tenosynovitis. J Hand Surg Eur Vol. 2015;40(7):720-728.
- Hyatt BT, Bagg MR. Flexor tenosynovitis. Orthop Clin North Am. 2017;48(2):217-227.
- Zhou JY, Mittermiller PA, Nishimoto SK, et al. Acute extensor tenosynovitis due to disseminated gonococcal infection. Plast Reconstr Surg Glob Open. 2019;7(9):e2432.
- Hubbard D, Joing S, Smith SW. Pyogenic flexor tenosynovitis by point-of-care ultrasound in the emergency department. Clin Pract Cases Emerg Med. 2018;2(3):235-240.
- Jardin E, Delord M, Aubry S, et al. Usefulness of ultrasound for the diagnosis of pyogenic flexor tenosynovitis: a prospective single-center study of 57 cases. Hand Surg Rehabil. 2018;37(2):95-98.
- Marvel BA, Budhram GR. Bedside ultrasound in the diagnosis of complex hand infections: a case series. J Emerg Med. 2015;48(1):63-68.
- Rice PA. Gonococcal arthritis (disseminated gonococcal infection). Infect Dis Clin North Am. 2005;19(4):853-861.




One Response to “Using Ultrasound to Diagnose Patient with Bilateral, Atraumatic Hand Pain”
June 6, 2021
SaraGreat case! Highlights the role of POCUS in honing the differential. As well as the need to obtain both genital AND throat swabs for suspected n. gonorrhea…